1. Position & Orientation – where exactly is the kidney?
- Location
- On the posterior abdominal wall, retroperitoneal (behind peritoneum).
- In the paravertebral gutter (close to the spine, not out at the flanks).
- Axis & hilum
- Long axis is parallel to the lateral border of psoas major.
- Because of a slight medial rotation, the hilum faces anteromedially (forwards & inwards).
- Level
- Hilum:
- Right – just below the transpyloric plane (L1).
- Left – just above the transpyloric plane (L1).
- Both are ~5 cm from the midline.
- Upper poles:
- Left → opposite 11th rib.
- Right → opposite 12th rib (right kidney lower because of the liver).
- Size & movement
- About 12 × 6 × 3 cm, weight 130–150 g.
- Moves ~2 cm vertically with respiration.
👉 If you can draw that in your mind, you can answer most “level/position” MCQs.
2. Posterior relations – the “bed” of the kidney

Think: “Diaphragm on top, then 3 muscles in a column”
From medial to lateral:
- Psoas major
- Quadratus lumborum
- Transversus abdominis aponeurosis
On top of these, covering the upper pole:
- The diaphragm (including fibres from the medial & lateral arcuate ligaments).
Important extra posterior relations:
- Above the diaphragm, a small costodiaphragmatic recess of pleura lies behind the upper pole → risk of pleural damage in posterior lumbar approach.
- Subcostal vein, artery & nerve + iliohypogastric & ilioinguinal nerves run behind the kidney after passing under the lateral arcuate ligament.
If they ask:
“Which structure is at risk in posterior approach to the kidney?”Answer: pleura (costodiaphragmatic recess).
3. Anterior relations – quick “organ list” you must know

Rather than memorising the entire paragraph, remember a clinical list for each side.
Right kidney – in front:
- Superior: Right suprarenal gland.
- Medial upper: Second part of duodenum (separates hilum from peritoneum).
- Upper anterior surface: Liver (→ hepatorenal pouch peritoneum).
- Lateral lower: Hepatic flexure of colon.
- Medial lower: Peritoneum, loops of jejunum.
“Right kidney lives under the LIVER, touches DUODENUM, COLON, and JEJUNUM — with SUPRA on top.”
Left kidney – in front:
- Superior: Left suprarenal gland.
- Medial upper:
- Stomach and lesser sac (part of the stomach bed).
- Body of pancreas + splenic vessels in front of the hilum.
- Lateral upper: Spleen (+ splenorenal ligament between them).
- Lateral lower: Splenic flexure of colon.
- Medial lower: Peritoneum + loops of jejunum.
If you can recall:
- Right: suprarenal, liver, duodenum, colon, jejunum
- Left: suprarenal, stomach, spleen, pancreas, colon, jejunum
→ that’s enough for most exams.
“Left kidney lies behind the STOMACH, SPLEEN, and PANCREAS — plus COLON and JEJUNUM — with SUPRA on top.”
4. Perinephric fat & renal fascia (Gerota) – why the kidney stays in place
Layers around the kidney (from inside out):
- Renal capsule – thin, firmly attached.
- Perinephric fat – directly outside capsule.
- Renal fascia (Gerota) – encloses kidney + perinephric fat.
- Paranephric fat – outside the fascia (not described here, but often added in exams).
Key points from the text:
- Perinephric fat
- Surrounds the kidney and helps hold it in position.
- Loss of this fat (e.g. severe weight loss) → nephroptosis (‘floating kidney’).
- Renal fascia (Gerota)
- A condensation of areolar tissue between parietal peritoneum and posterior abdominal wall.
- Forms a dome over the upper pole & suprarenal, but:
- A fascial septum separates kidney & suprarenal, so in nephrectomy the suprarenal is usually not displaced.
- Laterally: anterior & posterior layers fuse at the lateral border.
- At hilum: fascia attaches to renal vessels & ureter.
- Inferiorly: fades into extraperitoneal tissue around ureter.
Perinephric abscess behavior:
- Fascia tends to limit spread → abscess stays within perinephric space.
- With increasing pressure, fascia can rupture, allowing pus/injected fluid to track downwards retroperitoneally towards the pelvis.
👉 Exam line:
Renal fascia limits perinephric abscess; a fascial septum separates kidney from suprarenal.
5. Hilum & renal pelvis – what goes where
- Hilum = vertical slit on medial border:
- Transmits renal vein, renal artery, lymphatics, nerves & renal pelvis.
- Renal pelvis:
- Funnel-shaped beginning of the ureter.
- Normally the most posterior of the three main hilar structures (vein–artery–pelvis from front to back in many texts; here the key is “pelvis is posterior”).
- Capacity < 5 mL in normal state.
So if they ask:
In the hilum of the kidney, which structure lies most posteriorly?Answer: Renal pelvis (or beginning of the ureter).
6. One simple mental picture to lock it in
Imagine each kidney as:
- A bean stuck on the back wall of the abdomen:
- Tilted so its front edge is slightly turned towards you → that’s why the hilum faces anteromedially.
- Sitting on a bed of muscles:
- Psoas (medial), quadratus lumborum (middle), transversus abdominis (lateral).
- Wearing:
- A tight fat jacket (perinephric fat) inside a thin plastic bag (renal fascia) → this jacket + bag hold it in place and contain infection.
- On the head of each kidney sits a little cap = suprarenal gland.
- In front of each kidney:
- Right: mainly liver & duodenum & colon.
- Left: stomach, spleen, pancreas & colon.
If that picture is clear, anatomy viva becomes much easier.
Quick self-check (you can answer in your head)
- Which rib is related to the upper pole of:
- Right kidney?
- Left kidney?
- Name two major posterior structures that make the lumbar approach to the kidney risky.
- Which structure in the hilum is most posterior?
Answers (peek only after trying):
- Right – 12th rib; Left – 11th rib.
- Diaphragm + pleura (costodiaphragmatic recess); also subcostal vessels/nerves & iliohypogastric/ilioinguinal nerves behind.
- Renal pelvis (beginning of ureter).
KIDNEY — COMPLETE ANATOMY TABLE (ZERO-OMISSION)
1. Position, Orientation & Levels
Feature | Details |
Location | Posterior abdominal wall |
Peritoneal relation | Retroperitoneal |
Regional position | Paravertebral gutter |
Long axis | Parallel to lateral border of psoas major |
Hilum direction | Faces anteromedially (forward + inward) |
Reason for hilum direction | Slight medial rotation of kidney |
Hilum level (Right) | Just below transpyloric plane (L1) |
Hilum level (Left) | Just above transpyloric plane (L1) |
Distance from midline | ~5 cm |
Upper pole (Right) | Opposite 12th rib |
Upper pole (Left) | Opposite 11th rib |
Reason right kidney lower | Liver |
Size | 12 × 6 × 3 cm |
Weight | 130–150 g |
Respiratory movement | Moves ~2 cm vertically |
2. Posterior Relations (“Kidney Bed”)
Muscles (Medial → Lateral)
Order | Structure |
1 | Psoas major |
2 | Quadratus lumborum |
3 | Transversus abdominis aponeurosis |
Superior Posterior Relation
Structure | Notes |
Diaphragm | Covers upper pole |
Medial arcuate ligament | Diaphragmatic fibres |
Lateral arcuate ligament | Diaphragmatic fibres |
Structures at Risk Posteriorly
Structure | Clinical relevance |
Costodiaphragmatic recess of pleura | Risk in posterior lumbar approach |
Subcostal vein | Passes behind kidney |
Subcostal artery | Passes behind kidney |
Subcostal nerve | Passes behind kidney |
Iliohypogastric nerve | Passes behind kidney |
Ilioinguinal nerve | Passes behind kidney |
Classic exam answer (posterior approach risk):
➡ Pleura (costodiaphragmatic recess)
3. Anterior Relations — RIGHT Kidney
Region | Structure |
Superior | Right suprarenal gland |
Upper anterior surface | Liver |
Medial upper | Second part of duodenum |
Lateral lower | Hepatic flexure of colon |
Medial lower | Peritoneum + loops of jejunum |
Mnemonic logic:
Right kidney → Liver + Duodenum + Colon + Jejunum + Supra
4. Anterior Relations — LEFT Kidney
Region | Structure |
Superior | Left suprarenal gland |
Medial upper | Stomach |
Medial upper (behind stomach) | Lesser sac |
Hilum anterior | Body of pancreas |
Hilum anterior | Splenic vessels |
Lateral upper | Spleen |
Between spleen & kidney | Splenorenal ligament |
Lateral lower | Splenic flexure of colon |
Medial lower | Peritoneum + loops of jejunum |
Mnemonic logic:
Left kidney → Stomach + Spleen + Pancreas + Colon + Jejunum + Supra
5. Coverings of the Kidney (Inside → Outside)
Layer | Description |
1 | Renal capsule – thin, firmly adherent |
2 | Perinephric fat |
3 | Renal fascia (Gerota) |
4 | Paranephric fat |
6. Perinephric Fat — Key Points
Feature | Importance |
Function | Holds kidney in position |
Loss | Causes nephroptosis (floating kidney) |
Cause of loss | Severe weight loss |
7. Renal Fascia (Gerota) — Detailed Anatomy
Aspect | Detail |
Tissue type | Condensed areolar tissue |
Position | Between parietal peritoneum & posterior abdominal wall |
Encloses | Kidney + perinephric fat |
Superior extent | Forms dome over upper pole & suprarenal |
Kidney–suprarenal relation | Separated by fascial septum |
Nephrectomy implication | Suprarenal usually not displaced |
Lateral border | Anterior & posterior layers fuse |
At hilum | Attaches to renal vessels & ureter |
Inferiorly | Blends with extraperitoneal tissue around ureter |
8. Perinephric Abscess Behavior
Feature | Description |
Spread | Limited by renal fascia |
Usual location | Confined to perinephric space |
With high pressure | Fascia may rupture |
Direction of spread | Tracks downwards retroperitoneally to pelvis |
9. Hilum of Kidney
Feature | Description |
Position | Vertical slit on medial border |
Transmits | Renal vein, renal artery, lymphatics, nerves, renal pelvis |
Posterior-most structure | Renal pelvis / ureter |
10. Renal Pelvis
Feature | Detail |
Nature | Funnel-shaped |
Continuation | Beginning of ureter |
Position | Most posterior in hilum |
Capacity | < 5 mL (normal) |
11. Ultra–High-Yield Exam One-Liners
Question | Answer |
Kidney peritoneal relation | Retroperitoneal |
Structure most posterior in hilum | Renal pelvis |
Posterior approach danger | Pleura |
Right kidney lower because of | Liver |
Loss of perinephric fat causes | Nephroptosis |
Kidney–suprarenal separated by | Fascial septum |
12. One-Look Mental Map (Exam Lock)
Component | Image |
Position | Bean on posterior wall |
Bed | Psoas → QL → TA |
Covering | Fat jacket inside fascia |
Cap | Suprarenal gland |
Right front | Liver, duodenum, colon |
Left front | Stomach, spleen, pancreas |
ARTERIAL SUPPLY
1. Renal arteries – key facts
- Origin & flow
- Each kidney gets a large, wide-bore renal artery.
- Blood flow is > 1 L/min (about 20–25% of cardiac output).
- Renal arteries leave the abdominal aorta at right angles.
- They run behind the renal veins and also behind the pancreas (esp. left side).
👉 Exam idea:
Order at the hilum (front → back):
Vein → Artery → Pelvis (VAP)
So naturally:
- Renal arteries run behind renal veins
Behind pancreas (especially left):
- Pancreas lies anterior to the aorta
- Renal arteries arise from aorta
- Therefore they must pass behind pancreas to reach kidneys
2. Segmental arteries & renal segments
- Each kidney is divided into 5 arterial segments, each with its own segmental artery:
- Apical
- Upper (superior)
- Middle
- Lower (inferior)
- Posterior
- At/near the hilum, the renal artery divides into:
- Anterior division → supplies 4 segments:
- Apical, upper, middle, lower
- Posterior division → supplies posterior segment only.
- CRITICAL EXAM POINT:
- Segmental arteries are end arteries.
- There is no collateral circulation between segments via arteries.
- So if a segmental artery is blocked → that segment infarcts.
👉 Surgical consequence:
You can do segmental (partial) nephrectomy along segment boundaries because they’re arterially independent units.
Renal segments — make it UNFORGETTABLE
1️⃣ Lock the 5 segments as a fixed picture
Think of the kidney sliced like orange wedges 🍊 — each wedge has ONE pipe only.
Order (say it aloud):
👉 A U M L + P
- Apical
- Upper
- Middle
- Lower
- Posterior
🧠 Memory line:
“A UML P kidney” (sounds odd → sticks)
2️⃣ One split at the hilum — this is the KEY logic
At the hilum, renal artery does a clean Y-split:
- Anterior division → 4 front segments
- Apical
- Upper
- Middle
- Lower
- Posterior division → ONLY posterior segment
🧠 Picture this:
Front of kidney = busy (4 branches)
Back of kidney = lonely (1 branch)
3️⃣ The EXAM KILLER FACT (cement this 🔨)
Segmental arteries = END arteries
- ❌ No arterial anastomosis between segments
- ❌ No backup
- ❌ No sharing
🧠 One-line exam reflex:
“Block one segmental artery → that segment dies.”
If you remember nothing else, remember this.
4️⃣ Why surgeons LOVE this anatomy 🩺
Because each segment is an independent arterial island:
- You can remove one segment
- Without killing the rest of the kidney
👉 Segmental (partial) nephrectomy is possible
👉 Surgery follows segmental boundaries
🧠 Analogy:
Kidney = 5 apartments, each with its own water pipeShut one pipe → only that apartment suffers
3. Aberrant / accessory renal arteries – what they really are
- An aberrant / accessory renal artery (e.g. a vessel from aorta directly to the lower pole) is actually:
- A segmental artery with an unusual origin (persistence of a fetal vessel).
- Key points:
- Functionally it is a normal segmental artery.
- Often not accompanied by a matching vein.
- Very important in surgery: if you ligate it, that segment loses its blood supply → infarction or ischemia of that pole.
👉 MCQ-style thought:
A “lower polar artery from the aorta” = segmental artery.
Not a random extra; don’t casually cut it.
Think of the kidney as a 5-room house 🏠
- Each room = 1 renal segment
- Each room has its own water pipe
- NO inter-connections between rooms
→ that pipe is a segmental artery
→ segmental arteries are END arteries
🚨 Now the “Accessory / Aberrant” Trick
What it looks like:
- A vessel coming directly from the aorta
- Going straight to the lower pole
What it really is:
A normal segmental artery that never moved to the hilum during development
✔️ Fetal vessel that persisted
✔️ Unusual origin, normal function
🔒 One-Line Exam Lock (memorise this)
“Accessory renal artery = segmental end artery with abnormal origin.”
⚠️ Surgical Consequence (this is WHY examiners love it)
- Surgeon thinks: “Extra artery… cut it”
- Reality:
- You just cut the only artery to that segment
- Result → ischemia / infarction of that renal pole
👉 No collateral rescue ❌
👉 Segment dies 💀
🎯 MCQ Reflex Answer Pattern
- Lower polar artery from aorta
- Accessory renal artery
- Aberrant renal artery
Your brain should instantly say:
“Segmental END artery – do NOT ligate.”
4. Renal veins vs arteries – pattern & communications
- Arteries:
- Do not communicate between segments → no arterial collaterals.
- Veins:
- Do communicate between segments.
- Form a venous network, then 5–6 veins at the hilum.
- These finally join to form a single renal vein.
👉 Exam sentence:
Arterial segments are independent (no collaterals), but segmental veins freely anastomose before forming the single renal vein.
🧱 Think: Kidney = Apartment Block
🔴 Arteries = Private Water Pipes
- Each flat (segment) has its own pipe
- Pipes DO NOT connect to neighbours
- If one pipe is cut → that flat has no water
👉 No arterial collaterals
👉 End arteries
👉 Segmental infarction if cut
🔵 Veins = Common Drainage System
- Waste water from all flats mixes freely
- Many small drains interconnect
- They merge near the exit into 5–6 veins
- Finally become ONE renal vein
👉 Free venous anastomosis
👉 Pressure equalisation
👉 Safe mixing before exit
5. Order of structures in the hilum – front to back
Classic exam favourite:
From anterior → posterior:
- Renal vein
- Renal artery
- Renal pelvis / ureter
Mnemonic: V-A-U → “Vein, Artery, Ureter”.
This matches your text:
“The usual order of structures in the hilum of each kidney is vein, artery, ureter from front to back.”
LYMPHATIC & NERVE SUPPLY
1. Lymph drainage – one line you MUST know
- Kidney lymph → para-aortic (lumbar) nodes at L2
specifically at the level of origin of the renal arteries.
👉 Exam sentence in your head:
“Renal lymph drains to para-aortic nodes at L2, near the renal artery origin.”
That’s it. That’s the 80% for lymph.
Fix the LEVEL first (this is the trick)
- Renal arteries arise at L2
- Lymph follows arteries 🡒 always
So your brain should auto-connect:
Renal artery → L2 → lymph nodes there
2. Sympathetic supply – where from, where to, what it does
- Origin in spinal cord:
- Pathway:
- Preganglionic fibres → thoracic & lumbar splanchnic nerves
- Synapse in coeliac ganglion & renal ganglia.
- Postganglionic fibres → renal vessels & kidney.
- Function:
T12–L1 segments (preganglionic sympathetic cells).
Mainly vasomotor → control diameter of renal blood vessels, so they influence renal blood flow.
👉 Mental picture:
“T12–L1 → splanchnic nerves → coeliac/renal ganglia → kidney arteries (vasomotor).”
🔒 ONE-LINE CORE LOCK (say it aloud)
“Kidney sympathetic = T12–L1 → splanchnic → coeliac/renal ganglia → renal vessels → vasoconstriction.”
Repeat this 3 times.
🧠 WHY THIS MAKES SENSE (logic cement)
1️⃣ Origin: T12–L1
- Kidney sits high (T12–L3 level).
- Sympathetic outflow always comes from thoracolumbar cord.
- So T12–L1 fits perfectly.
👉 If you see kidney, your brain should auto-jump to T12–L1.
2️⃣ Pathway: Splanchnic nerves
- Splanchnic nerves = highway nerves carrying sympathetic fibres to abdominal organs.
- Kidney is an abdominal organ → must use thoracic/lumbar splanchnics.
👉 Think: “No splanchnic = no abdominal sympathetic.”
3️⃣ Ganglia: Coeliac + Renal
- Kidney vessels branch near the coeliac axis.
- So fibres synapse in:
- Coeliac ganglion
- Renal ganglia
👉 Exam trick: kidney ≠ pelvic organ → NOT hypogastric plexus.
4️⃣ Target: Renal vessels
- Postganglionic fibres run along arteries.
- Sympathetic nerves love blood vessels.
👉 Visual: nerves hugging renal arteries like ivy.
5️⃣ Function: Vasomotor
- Sympathetic = vasoconstriction.
- Vasoconstriction → ↓ renal blood flow → ↓ urine output.
- Happens in:
- Shock
- Stress
- Exercise
- Hemorrhage
👉 Body logic: “Save blood for brain & heart — squeeze kidney vessels.”
🎯 EXAM TRIGGER PHRASES (auto-recall)
- Sympathetic kidney question? → Answer = VASOMOTOR
- Asked about secretion/micturition? → ❌ not sympathetic
- Asked about blood flow control? → ✅ sympathetic
🖼️ FINAL MENTAL PICTURE (burn it in)
Picture a red spinal cord at T12–L1
⬇
White splanchnic cables diving forward
⬇
Stopping briefly at coeliac/renal ganglia
⬇
Then wrapping tightly around renal arteries, squeezing them.
🔁 FINAL RAPID RECALL (last lock)
T12–L1 → splanchnic → coeliac/renal ganglia → renal vessels → vasoconstriction
3. Pain pathway in renal colic – “loin to groin”
Source: stone in calyces or renal pelvis → stretches system → pain.
Pathway of pain fibres:
- From kidney → coeliac plexus
- Then via thoracic & lumbar splanchnic nerves
- To sympathetic trunk
- Through white rami communicantes
- Into T12–L1 spinal nerves
- Into spinal cord via posterior roots
So the cord levels for kidney pain = T12–L1.
Referred pain pattern:
- Can be felt in:
- Back and lumbar region (loin)
- Anterior abdominal wall
- Radiating down towards external genitalia
→ the classic “loin to groin” description.
👉 So if a patient has flank pain radiating to groin, think renal/ureteric colic (T12–L1).
🎬 The movie in your head
- Stone stuck in renal pelvis / calyx
- Pain signal rides WITH sympathetic nerves (this is the key rule)
- Imagine the signal climbing UP the kidney vessels to the coeliac plexus
- From there it travels backwards:
- via thoracic & lumbar splanchnic nerves
- into the sympathetic trunk
- sneaks through white rami communicantes
- enters T12–L1 spinal nerves
- reaches the cord via posterior roots
→ urine backs up
→ stretching pain (this is the trigger)
(like electricity going back along a cable)
👉 STOP the movie here
👉 Lock the level: T12–L1
🧭 Why “loin → groin” happens (this is the examiner’s favourite WHY)
Think DERMATOMES, not organs.
- T12–L1 dermatomes supply:
- Flank / loin
- Lower anterior abdominal wall
- Groin
- External genitalia (via ilioinguinal & genitofemoral territory)
So the brain misreads visceral pain as coming from skin areas supplied by the same spinal segments.
🧠 Ultra-short memory locks (use whichever clicks)
🔑 Lock 1 – Sentence
“Kidney pain speaks T12–L1, so the pain walks from loin to groin.”
🔑 Lock 2 – Number hook
- Kidney pain = 12 + 1 = 13
- Think “Unlucky 13 = stone pain”
🔑 Lock 3 – Pathway shorthand (exam-safe)
Kidney → Coeliac plexus → Splanchnic nerves → White rami → T12–L1
🚨 Rapid exam reflex (automatic answer)
Question:
Patient with severe flank pain radiating to groin — nerve roots involved?
Reflex answer (no thinking):
T12–L1 (renal / ureteric colic)
4. Why nausea & vomiting with renal colic?
- There may be some afferent fibres travelling with the vagus.
- This could explain nausea and vomiting that often accompanies renal pain.
STRUCTURE
1. Gross structure – cortex, medulla, pyramids & calyces
When you cut the kidney longitudinally:
- Just under the capsule = cortex (dark reddish).
- Inside = medulla, arranged as triangular, striated pyramids.
Key relationships:
- Cortex:
- Forms outer band under capsule.
- Sends “columns” in between pyramids → renal columns.
- Medulla:
- Consists of renal pyramids.
- Each pyramid has an apex = renal papilla.
- Several pyramids can drain into one papilla.
- Drainage pathway (very exam-friendly):
- 1 Papilla opens into a 1 minor calyx.
- Minor calyces → join to form 2–3 major calyces.
- Major calyces → join to form the renal pelvis.
- Pelvis continues as ureter.
If you can say:
“Cortex outside, pyramids inside, papilla → minor calyx → major calyx → pelvis → ureter”you already have most MCQ marks for gross internal structure.
🎯 One fixed mental model (this must not change)
Imagine the kidney as a funnel system carved inside a solid organ
Step-by-step movie:
- Outer dark shell = Cortex
- Just under the capsule
- Think: filtering zone
- Not smooth inside — it dips between pyramids
- Those dips are renal columns
- Cortex going inward
- Columns separate pyramids
- Exam phrase: “cortical tissue extending between pyramids”
- Inside core = Medulla
- Made of triangular pyramids
- Striated → lines point towards the centre
- Tip of each pyramid = Papilla
- This is the dripping point
- Urine exits here
🚿 Drainage logic (THIS is the examiner’s gold)
Think small → bigger → bigger → tube
Lock this sequence permanently:
Papilla → Minor calyx → Major calyx → Renal pelvis → UreterWhy it’s impossible to forget:
- Papilla = single point
- Minor calyx = first cup
- Major calyx = joined cups (2–3 only)
- Pelvis = big funnel
- Ureter = pipe leaving kidney
🔐 Memory locks (choose 2, not all)
🔑 Lock 1 – Sentence (say it fast)
“Cortex outside, pyramids inside; papilla to calyx to pelvis to ureter.”🔑 Lock 2 – Shape logic
- Triangle = pyramid
- Point of triangle = papilla
- Cup catches drip = calyx
- Funnel = pelvis
- Pipe = ureter
(Your brain remembers shapes better than words.)
🔑 Lock 3 – Exam reflex
If asked “gross internal structure of kidney”, your mouth should auto-say:
“Outer cortex with renal columns; inner medulla arranged as pyramids whose papillae drain into minor calyces, then major calyces, forming the renal pelvis which continues as ureter.”That single sentence covers everything you wrote.
🚨 Common examiner traps (avoid silently)
- ❌ Saying papilla → major calyx (minor comes first)
- ❌ Forgetting renal columns (easy viva mark)
- ❌ Saying each pyramid has its own papilla (❌ — several pyramids may share)
🧠 Final compression (ultimate exam line)
The kidney has an outer cortex that extends inward as renal columns between medullary pyramids; each pyramid ends in a papilla that drains into a minor calyx, which joins major calyces to form the renal pelvis, continuing as the ureter.
2. Nephron – the basic functional unit (what it is + where it sits)
- Nephron = functional & histological unit of kidney.
- About 1 million nephrons per kidney.
Main parts in order:
- Glomerulus:
- Tuft of capillaries.
- Wrapped by Bowman’s capsule lined by special epithelial cells called podocytes.
- Space inside Bowman’s capsule receives the glomerular filtrate (deproteinized plasma).
- Tubule system (continuous with Bowman’s capsule epithelium):
- Proximal convoluted tubule (PCT) – directly from Bowman’s.
- Loop of Henle – thin-walled, dips into medulla.
- Distal convoluted tubule (DCT).
- Collecting tubule → collecting duct.
Location by region:
- Cortex:
- Glomeruli
- Proximal convoluted tubules
- Distal convoluted tubules
- Medulla:
- Loops of Henle
- Collecting tubules & collecting ducts
Collecting ducts → unite → largest open at tip of papilla into minor calyx.
👉 Exam picture in your mind:
Cortex = “filters + coiled tubes” (glomeruli + PCT + DCT).
Medulla = “straight tubes going up & down” (loops + collecting ducts).
3. Blood around the nephron – afferent, efferent, peritubular
- Glomerular capillaries are fed by an afferent arteriole.
- They drain into an efferent arteriole (important: arteriole → capillary → arteriole).
- Efferent arteriole then breaks up into peritubular capillaries around the PCT & DCT.
This blood supply allows:
- Filtration at glomerulus → filtrate in Bowman’s capsule.
- Reabsorption & secretion in tubules via peritubular capillaries.
Definition of urine here:
Urine = glomerular filtrate (deproteinized plasma) that has been modified by selective reabsorption + secretion along the tubules.
4. Juxtaglomerular apparatus – renin source 🩺
- Certain arteriolar cells (especially from afferent arteriole) + DCT cells together form the juxtaglomerular (JG) apparatus.
- Function: secretes renin, which is key in blood pressure and volume control (RAAS).
Exam tip:
“Where is renin produced?” → juxtaglomerular apparatus in the kidney.
5. Pelvis & calyces – epithelium + pacemaker function
- Pelvis and ureter are lined by transitional epithelium (urothelium).
- Their walls contain smooth muscle.
Special point:
- Specialized muscle cells in the walls of the minor calyces act as pacemakers.
- They initiate peristaltic waves that travel down the pelvis into the ureter, propelling urine.
👉 So urine doesn’t “fall”; it is actively pushed by peristalsis starting in the calyces.
🧠 One CORE IDEA (don’t split it)
Urine is ACTIVELY DRIVEN, not passively drained.
Everything else hangs on this.
🔗 Build the logic in the correct order
1️⃣ Lining (structure → function)
- Pelvis + calyces + ureter
→ lined by transitional epithelium (urothelium)
Why this matters:
- Can stretch as urine volume changes
- Protects underlying tissue from urine toxicity
👉 This lining tells you: dynamic system, not a rigid pipe
2️⃣ Wall (the engine)
- Walls contain smooth muscle
- Smooth muscle = involuntary, rhythmic contraction
👉 No skeletal muscle here → no voluntary control
3️⃣ The KEY EXAM POINT (pacemaker)
This is where most people fail.
- Specialised smooth muscle cells
- Located in walls of the MINOR CALYCES
- They act as PACEMAKERS
Think like the heart:
- SA node starts rhythm
- Wave spreads forward
Here:
- Minor calyx starts the wave
- Wave spreads → renal pelvis → ureter
🚿 How urine actually moves (step-by-step movie)
🎬 Movie in your head:
- Urine drips from papilla into minor calyx
- Pacemaker cells fire
- Peristaltic wave starts
- Wave travels:
- Minor calyx
- Major calyx
- Renal pelvis
- Ureter
- Urine is pushed forward, even:
- Against gravity
- In lying-down patients
👉 So urine never “falls”
🔐 Memory locks (use 2 max)
🔑 Lock 1 – Sentence (exam reflex)
“Peristalsis of urine starts in the minor calyces due to pacemaker smooth muscle cells.”
🔑 Lock 2 – Analogy
- Minor calyx = SA node
- Pelvis & ureter = conduction pathway
Once started, the wave must move forward.
🚨 Common examiner traps (avoid silently)
- ❌ Saying peristalsis starts in the ureter
- ❌ Saying urine flows by gravity
- ❌ Forgetting smooth muscle
- ❌ Forgetting transitional epithelium
🧠 Ultimate one-line exam answer (this alone scores)
The renal pelvis and calyces are lined by transitional epithelium and contain smooth muscle, with specialised pacemaker cells in the minor calyces initiating peristaltic waves that propel urine through the pelvis into the ureter.
DEVELOPMENT
1. Three “kidneys” in development – which one becomes adult kidney?
In order (cranial → caudal):
- Pronephros
- Very rudimentary & transient (“evanescent”).
- Its duct persists.
- Mesonephros
- Has segmentally arranged tubules.
- Tubules open into the pronephric duct, which then becomes the mesonephric (Wolffian) duct.
- Metanephros = definitive adult kidney
- Formed caudally from intermediate cell mass, giving rise to ~1 million tubules.
- These tubules = metanephric blastema → form nephrons (Bowman’s capsule, PCT, loop, DCT).
👉 Key idea:
- Duct system (collecting system) comes from ureteric bud.
- Secretory units (nephrons) come from metanephric tissue.
If you say that in viva, you’re already sounding like you know what you’re doing.
2. Ureteric bud – the branching tree & what it forms
- Ureteric bud:
- Grows out from the caudal end of the mesonephric (Wolffian) duct.
- Separates from the mesonephric duct later.
- What the ureteric bud forms:
- Ureter
- Renal pelvis
- Major calyces
- Minor calyces
- Collecting tubules & collecting ducts of medullary pyramids
- Meanwhile, distal convoluted tubules of the metanephric nephrons grow to join the collecting system.
Extra link:
- The mesonephric duct (after bud separates) contributes to:
- Bladder (part of it).
- In male → vas deferens + associated structures.
👉 Mental picture:
- Wolffian duct = “old pipe” that sprouts a side branch (ureteric bud) → builds the whole collecting system tree.
- Metanephric tissue = “grapes” (nephrons) plugging into the tips of that tree.
3. Ascent & blood supply – how the kidney ends up in the lumbar region
- Metanephros (definitive kidney) starts in the pelvis.
- Initially supplied by branches from the internal iliac artery.
- As it ascends:
- It gets new arteries from common iliac and later aorta.
- Older vessels usually regress.
- Eventually, you’re left with a (usually) single renal artery from the aorta.
- Hilum orientation:
- Initially faces anteriorly.
- During ascent, kidney rotates ~90° medially, so the hilum faces anteromedially (adult position).
👉 Very exam-y sentence:
“Metanephros arises in pelvis, ascends to lumbar region, changing its arterial supply stepwise from internal iliac → common iliac → aorta, with 90° medial rotation of the hilum.”
4. Fetal lobulation – just a normal developmental look
- Fetal & neonatal kidneys appear lobulated.
- This reflects metanephric tissue capping each ureteric bud branch.
- Persistence of fetal lobulation in adults is common and has no clinical significance.
5. Main anomalies – the ones examiners like
a) Persistent fetal arteries (accessory renal arteries)
- Because the kidney acquires new arteries as it ascends, one of the earlier arteries may persist.
- Common: an artery from the aorta to the lower pole.
- These are actually segmental arteries with unusual origins.
- Common (about 30% of individuals).
Clinical point:
- If you ligate one of these by mistake, the segment it supplies can infarct.
b) Horseshoe kidney
- Fusion of lower poles of the two kidneys → horseshoe-shaped organ.
- Occurs in about 1 in 800.
- The fused isthmus:
- Lies anterior to the aorta.
- Ureters pass anterior to the isthmus.
- Ascent is limited because the isthmus gets caught under the inferior mesenteric artery (IMA) → kidney remains lower than normal.
👉 Classic exam line:
“Horseshoe kidney fails to ascend fully because the fused lower poles are trapped under the IMA.”
c) Polycystic kidney disease (PKD)
- Occurs in about 1 in 500.
- Both kidneys studded with multiple cysts.
- It is hereditary.
- Can be associated with cysts in liver, pancreas, lungs.
d) Renal agenesis (single kidney)
- Around 1 in 500 people have only one kidney (unilateral renal agenesis).
- Clinically critical point:
- Must be ruled out before nephrectomy – don’t remove the only kidney.
SURGICAL APPROACH
1. Lumbar approach – how & why
Used for:
- Nephrectomy (removal of kidney)
- Nephrolithotomy (removal of stones)
Key steps & ideas:
- Approach from the back (lumbar) → avoids opening the peritoneal cavity.
- Surgeon incises renal fascia + perinephric fat → exposes kidney.
- Upper pole is freed, but suprarenal gland is left behind in its own fascial compartment
- Peritoneum is pushed forwards and medially → keeps abdominal contents out of the way.
- Renal vessels:
- Exposed at hilum.
- Ligated and divided – ARTERY BEFORE VEIN
- Right side special risk:
- Right kidney may adhere to colon, duodenum, IVC, suprarenal.
- Right renal vein is only ~2.5 cm → IVC is very close to operative field.
- Left side adhesions:
- To colon, spleen, pancreas, suprarenal.
- Now also done via laparoscopic (minimal access) methods, but basic anatomy logic is the same.
➝ Because kidney & suprarenal are separated by a fascial septum.
(standard rule to prevent kidney congestion/swelling).
👉 If you remember:
“Lumbar approach, open fascia/fat, leave suprarenal, push peritoneum away, ligate artery then vein, beware short right renal vein near IVC,”you’ll answer most surgical-approach questions.
2. Percutaneous renal biopsy – safe entry point + main danger
Target: usually lower pole of the kidney.
Approach:
- Needle is inserted:
- About 2.5 cm below the 12th rib
- Distance from midline decided radiologically (imaging-guided).
Risks:
- Possible damage to a renal vessel or a calyx → bleeding or haematuria.
Important technical point:
- Needle is only advanced while the patient holds their breath
➝ So the kidney doesn’t move with respiration and get torn by needle.
👉 Key memory:
“Biopsy → lower pole, 2.5 cm below 12th rib, imaging-guided, risk = vessel/calyx injury, advance needle only on breath-hold.”
3. Renal transplantation – where the new kidney lives
Site:
- Donor kidney is placed retroperitoneally in the iliac fossa (usually right side).
Orientation:
- Hilum is kept parallel to the external iliac vessels.
Vascular anastomoses:
- Renal artery → joined to internal or external iliac artery.
- Renal vein → joined to external iliac vein.
Ureter:
- Ureter is implanted directly into the bladder.
👉 So for viva/MCQ:
“Transplant kidney goes into the iliac fossa, retroperitoneal; renal artery to internal/external iliac artery, renal vein to external iliac vein, ureter into bladder.”
URETER(abdominal part)
1. Basics + 3 narrowest points (STONE SITES)
- Length: about 25 cm.
- Three physiologic narrowings (classically where stones lodge):
- Pelvi-ureteric junction (PUJ) – where renal pelvis becomes ureter.
- Where it crosses the pelvic brim – at the bifurcation of the common iliac artery / sacroiliac joint.
- Where it passes through the bladder wall (vesicoureteric junction).
👉 If you remember “PUJ – pelvic brim – bladder wall” you’ve already got a big chunk of ureter MCQs.
Mental Story (works extremely well for exams)
- PUJ = First Gate (Mountain Exit)
- Imagine urine leaving the renal pelvis through a narrow mountain pass.
- Stones get stuck right at the start.
- 👉 Pelvis → Ureter = sudden narrowing
- Pelvic Brim = Second Gate (Road Crossing)
- The ureter is cruising down, then suddenly crosses a hard bony ridge.
- Right here it crosses the common iliac artery bifurcation.
- 👉 Stone hits the “speed breaker” at the pelvic brim
- Bladder Wall = Final Gate (Tunnel Entry)
- Ureter pierces the bladder wall obliquely.
- This part is tight + compressed during bladder filling.
- 👉 Stone stuck just before entering bladder
🔒 Ultra-solid exam lock
“PUJ → Pelvic brim → Bladder wall”
Say it like a journey:
- Start (PUJ)
- Midway obstacle (pelvic brim)
- Finish line gate (VUJ)
🩺 Why examiners LOVE this
- These are physiological, not random.
- They explain:
- Typical renal colic pain migration
- X-ray / CT stone locations
- Hydronephrosis patterns
2. Abdominal course – what it runs on & what crosses it

Core pathway
- Ureter runs down on psoas major, under cover of peritoneum.
- It lies:
- In front of the genitofemoral nerve.
- Is itself crossed anteriorly by the gonadal vessels.
👉 Classic viva phrase:
“The ureter lies on psoas major, anterior to genitofemoral nerve, and is crossed anteriorly by gonadal vessels.”
Right vs left (just the big ideas)
You don’t need every vessel, just the key trends:
- Right ureter:
- Upper part: behind the 3rd part of the duodenum.
- Lower down: crossed anteriorly by:
- Right colic vessels
- Ileocolic vessels
- Root of mesentery
- Left ureter:
- Lateral to inferior mesenteric vessels.
- Crossed anteriorly by:
- Left colic vessels
- Apex of sigmoid mesocolon at pelvic brim
At the pelvic brim (both sides):
- It leaves psoas and crosses:
- Over the sacroiliac joint
- At the bifurcation of the common iliac artery
- To enter the pelvis.

🧠 CORE FIXED IMAGE (never change this)
Imagine the ureter as a white tube sliding down a muscle slope.
🔹 The slope = psoas major
- Ureter rests ON psoas major
- Covered by peritoneum → retroperitoneal
👉 Base picture:
“White tube sliding down psoas under peritoneum.”
This image alone anchors everything else.
🧠 RELATION TRIANGLE (3 things only — exam safe)
Now freeze these three relations around the ureter:
1️⃣ Behind it (posterior):
- Psoas major
- Genitofemoral nerve (running on psoas)
👉 Lock:
Ureter is ANTERIOR to genitofemoral nerve.
2️⃣ In front of it (anterior):
- Gonadal vessels (testicular / ovarian)
👉 Classic examiner line:
“Gonadal vessels cross the ureter anteriorly at L3,4 level.”
3️⃣ Covering it:
- Peritoneum
📌 One-line lock (must be reflex):
On psoas – anterior to genitofemoral nerve – crossed anteriorly by gonadal vessels
If you can say this in 3 seconds → you’re safe.
🧠 RIGHT vs LEFT — don’t memorize, VISUALIZE FLOW
🟢 RIGHT URETER = “duodenum + mesentery side”
Picture the right ureter passing behind gut structures.
- Upper right ureter
- Behind 3rd part of duodenum ✅ (very testable)
- Lower right ureter gets crossed anteriorly by:
- Right colic vessels
- Ileocolic vessels
- Root of mesentery
👉 Mental phrase:
“Right ureter = behind duodenum, under mesentery vessels.”
🔵 LEFT URETER = “sigmoid + IMA side”
Left side is colon-heavy.
- Lies lateral to inferior mesenteric vessels
- Crossed anteriorly by:
- Left colic vessels
- Apex of sigmoid mesocolon (key pelvic brim relation)
👉 Mental phrase:
“Left ureter = lateral to IMA, under sigmoid mesocolon.”
🧠 PELVIC BRIM — UNIVERSAL LOCK (both sides)
This is non-negotiable exam material.
At pelvic brim, the ureter:
- Leaves psoas major
- Crosses:
- Sacroiliac joint
- Bifurcation of common iliac artery
- Then enters pelvis
📌 Stone + anatomy lock:
“Ureter crosses common iliac bifurcation at sacroiliac joint.”
This is why stones get stuck here.
🎯 FINAL ONE-LINE SUPERLOCK (repeat till reflex)
“The ureter runs retroperitoneally on psoas major, anterior to the genitofemoral nerve, crossed anteriorly by gonadal vessels; on the right it passes behind the 3rd part of the duodenum and mesentery, on the left lateral to inferior mesenteric vessels and sigmoid mesocolon, and at the pelvic brim it crosses the common iliac bifurcation over the sacroiliac joint.”
3. How to recognise ureter in surgery (super practical line)
In the living body, ureter =:
- Whitish
- Non-pulsatile
- Cord-like
- Shows visible peristaltic waves when gently pinched with forceps.
👉 That’s the textbook phrase examiners love.
4. Surface marking & X-ray projection – only what you really need
Surface mark (front of abdomen)
- On the anterior abdominal wall, abdominal ureter lies on a line:
- From tip of 9th costal cartilage
- To bifurcation of the common iliac artery.
(That’s mainly for old-school clinical palpation & KUB interpretation.)
Radiographic projection (on a plain film)
- In the abdomen:
- Ureter runs medial to the tips of the transverse processes of lumbar vertebrae.
- At pelvic brim:
- Crosses at the sacroiliac joint (key landmark).
- In the pelvis:
- Shadow passes towards the ischial spine
- Then (foreshortened) towards the pubic tubercle.
👉 So on X-ray, think:
“Medial to transverse process tips → crosses SI joint → ischial spine → pubic tubercle.”
🔒 ONE CORE MENTAL TRACK (X-ray Pathway)
Say this out loud every time:
“Medial → SI → Spine → Pubis”
That single line is the entire radiographic ureter course.
🧠 STEP-BY-STEP VISUAL LOCK (Plain X-ray / KUB)
1️⃣ Abdomen (lumbar spine level)
- Ureter shadow lies medial to the tips of lumbar transverse processes
- Never lateral → this avoids confusing it with bowel gas
🧠 Hook:
👉 “Ureter hugs the spine, not the flank.”
2️⃣ Pelvic brim (MOST TESTED POINT)
- Crosses exactly at the sacroiliac (SI) joint
🧠 Exam lock:
👉 Stone at pelvic brim = SI joint level.
3️⃣ Pelvis (after entering)
- Runs towards ischial spine
🧠 Hook:
👉 “Ureter aims for the spine before the pubis.”
4️⃣ Terminal foreshortened part
- Turns medially & inferiorly towards pubic tubercle
- Looks shortened on X-ray because it’s entering bladder wall
🧠 Hook:
👉 “Ends short because it dives into bladder.”
🎯 ULTRA-COMPACT EXAM LINE (MEMORISE)
On plain X-ray, the ureter runs medial to lumbar transverse process tips, crosses the sacroiliac joint, passes towards the ischial spine, and ends foreshortened near the pubic tubercle.
🧲 5-SECOND RAPID RECALL (use in viva)
Question:
“Describe ureter course on X-ray.”
Answer:
👉 “Medial to transverse processes → SI joint → ischial spine → pubic tubercle
BLOOD,NERVE,LYMPH SUPPLY OF URETER
1. Blood supply – segmental + KEY surgical point
a) Who supplies what?
Think in three zones:
- Upper ureter
- Middle ureter
- Abdominal aorta
- Gonadal artery (testicular/ovarian)
- Common iliac artery
- Internal iliac artery
- Lower ureter
- Superior vesical artery
- Inferior vesical artery (in male)
- Uterine artery (in female)
→ Ureteric branches of renal artery
→ Small branches from:
→ Branches from:
👉 Mental picture:
Kidney side → renal artery
pelvis side → vesical/uterine
in between → aorta + gonadal + iliacs.
🧠 ONE MASTER IDEA (DON’T LET GO)
Ureter blood supply = SEGMENTAL + LONGITUDINAL
👉 Many small arteries → run along ureter → NO single dominant trunk
That is the surgical danger.
🎯 THE ONLY 3-ZONE LOGIC YOU NEED
Say this slowly in your head:
“Top = Kidney, Bottom = Bladder/Uterus, Middle = Everything in between.”
Now expand 👇
🔵 1️⃣ UPPER URETER (Kidney side)
- Supplied by:
- Ureteric branches of renal artery
🧠 Brain hook:
👉 Upper ureter lives in kidney territory → renal artery feeds it.
🟡 2️⃣ MIDDLE URETER (The “messy” zone)
Supplied by multiple small feeders:
- Abdominal aorta
- Gonadal artery (testicular / ovarian)
- Common iliac artery
- Internal iliac artery
🧠 Ultra-simple hook:
👉 Middle ureter grabs blood from anything it passes.
Or even simpler:
👉 “Aorta + Gonadal + Iliacs”
🔴 3️⃣ LOWER URETER (Pelvic / bladder side)
- Superior vesical artery
- Inferior vesical artery (♂ male)
- Uterine artery (♀ female)
🧠 Golden exam line:
👉 “Water under the bridge”
Ureter under uterine artery → uterine artery supplies it.
🧲 ONE-LINE MEMORY LOCK (SMALL BRAIN VERSION)
Top = Renal, Middle = Aorta + Gonadal + Iliacs, Bottom = Vesical / Uterine.
Say it 3 times. That’s enough.
⚠️ KEY SURGICAL POINT (VERY HIGH YIELD)
🚨 Ureteric arteries are:
- Small
- Multiple
- Segmental
- End arteries
❌ If you strip ureter → ischemia → necrosis → stricture → fistula
🧠 Surgical mantra:
👉 “Never skeletonise the ureter.”
🧠 FINAL 5-SECOND EXAM ANSWER
Q: Blood supply of ureter?
👉 “Segmental supply: upper from renal artery, middle from aorta, gonadal and iliac branches, lower from vesical arteries and uterine artery in females.”
b) Anastomosis & surgical danger
- All these little arteries anastomose in the adventitia of the ureter, forming longitudinal channels along its length.
- VERY important surgical point:
- If you strip the ureter clean of its surrounding tissue (“skeletonize” it)
➝ you destroy those adventitial vessels
➝ risk ischemia and necrosis of ureter.
So in surgery:
Always mobilize ureter with its sheath, not bare.
🧠 THE ONE CORE TRUTH (LOCK THIS FIRST)
Ureter survives on its adventitia.
Not the lumen.
Not one big artery.
👉 The adventitial sheath is life.
🔗 HOW THE BLOOD REALLY RUNS (PICTURE THIS)
- Many tiny segmental arteries reach the ureter
- They join together in the adventitia
- They form longitudinal vascular channels running up and down the ureter
🧠 Mental image:
👉 A cable wrapped with tiny wires along its outer insulation.
⚠️ THE SURGICAL DISASTER (EXAM GOLD)
What happens if you skeletonize the ureter?
- You strip off the adventitia
- You cut the longitudinal anastomotic channels
- Blood supply is not replaced
- Result:
- Ischemia
- Necrosis
- Stricture
- Urinary fistula
🧠 Brutal memory hook:
👉 Bare ureter = dead ureter.
🧠 ONE-LINE VIVA ANSWER (PERFECT)
“Ureteric arteries anastomose longitudinally in the adventitia; skeletonization destroys these vessels and risks ischemic necrosis, so the ureter must be mobilized with its sheath.”
Say it once. Examiner nods.
🧲 MICRO-MNEMONIC (SMALL BRAIN MODE)
A-L-I-V-E
- Adventitia
- Longitudinal vessels
- Ischaemia if stripped
- Viable only with sheath
- End-artery danger
🏁 FINAL SURGICAL COMMANDMENT (NEVER FORGET)
“Always mobilize the ureter WITH its sheath, never bare.”
2. Lymph drainage – simple split
Lymphatics follow arteries:
- Abdominal ureter → para-aortic (lumbar) nodes.
- Pelvic ureter → common iliac & internal iliac nodes.
You can link it to what you already know:
- Kidney & upper ureter → para-aortic
- Pelvic structures → iliac nodes.
🧠 Core Rule (say this first, every time)
“Lymph follows arteries.”
If you know where the artery drains, you know where the lymph goes.
🧱 Step 1: Split the ureter into TWO worlds
🔹 World 1: Abdominal ureter
- Location: above pelvic brim
- Blood supply: direct branches from aorta
- Therefore lymph goes to → para-aortic (lumbar) nodes
👉 Concrete sentence
“Anything fed by the aorta drains to para-aortic nodes.”
🔹 World 2: Pelvic ureter
- Location: below pelvic brim
- Blood supply: iliac arteries
- Therefore lymph goes to →
common iliac + internal iliac nodes
👉 Concrete sentence
“Anything living in the pelvis drains to iliac nodes.”
🧠 Step 2: One visual picture (VERY important)
Imagine this:
- 🛣️ AORTA = highway
- Things alongside it → para-aortic nodes
- 🚦 PELVIC BRIM = border checkpoint
- Once crossed → iliac territory
👉 Ureter crosses pelvic brim = lymph drainage changes
🔒 Step 3: Exam-lock phrases (repeat these)
- Kidney + upper ureter → para-aortic
- Pelvic ureter → iliac nodes
- Pelvis = iliac
- Aorta = para-aortic
If stuck in an exam, ask yourself:
“Is this structure fed by the aorta or iliac arteries?”
The answer gives you the lymph node automatically.
🎯 Ultra-short MCQ reflex line
“Ureter lymph: above brim → para-aortic; below brim → iliac.”
Say it once now.
Say it again before sleep.
This one won’t leave your head.
3. Nerve supply – what matters vs what doesn’t
- Sympathetic fibres:
- From T10–L1 spinal segments.
- Reach ureter via coeliac plexus & hypogastric plexus.
- Parasympathetic fibres:
- From pelvic splanchnic nerves (S2–S4).
BUT big exam idea:
- Peristalsis of ureter does not depend on innervation.
- It is started by pacemaker cells in calyces/renal pelvis.
- Ureter can still propagate peristaltic waves even if its extrinsic innervation is cut.
- No ganglion cells in or on ureter (unlike gut).
- Pain fibres:
- Run with sympathetics (like kidney).
- So ureteric colic pain refers to similar T10–L1 dermatomes → flank → groin.
🧠 ONE CORE IDEA (burn this first)
Ureter = self-driving tube. Nerves modify sensation, NOT movement.
If you remember only this, you’ll never get trapped in MCQs.
🚦 Split it into 3 mental boxes
① Movement (Peristalsis) → NOT nerve-dependent
Picture this 👇
- Pacemaker cells sit in calyces + renal pelvis
- They initiate peristalsis
- Wave propagates down ureter automatically
🔒 Concrete lock:
✂️ Cut all ureteric nerves → urine STILL moves
So:
- ❌ Sympathetic = NOT essential for peristalsis
- ❌ Parasympathetic = NOT essential for peristalsis
This is EXACTLY unlike gut.
② Innervation → sensory & modulation only
🔴 Sympathetic fibres
- From T10–L1
- Travel via:
- Coeliac plexus
- Hypogastric plexus
- Role:
- Carry pain
- Minor tone modulation (not propulsion)
🔵 Parasympathetic fibres
- From pelvic splanchnic nerves (S2–S4)
- Minor influence only
- Not required for peristalsis
🔒 Exam sentence:
“Ureteric peristalsis is intrinsic and independent of extrinsic autonomic innervation.”
③ Pain (THIS is what nerves really matter for)
This is the exam gold 🥇
- Pain fibres run with sympathetic nerves
- Same rule as kidney
So:
- Origin: T10–L1
- Referred pain:
- Flank → loin → groin
- Can go to scrotum / labia
🔒 Pain lock phrase:
“Ureteric colic pain follows sympathetics → T10–L1 dermatomes.”
❗ Extra exam trap to avoid
- ❌ NO ganglion cells in or on ureter
- ❌ Do NOT compare ureter to gut ENS
🔒 One-line contrast:
Gut has intrinsic ganglia; ureter has intrinsic pacemaker cells — not neurons.
🧠 FINAL 5-LINE MEMORY BLOCK (repeat this)
- Ureter moves urine by intrinsic pacemaker-driven peristalsis
- Movement does not need nerves
- Sympathetic (T10–L1) & parasympathetic (S2–S4) are modulatory
- Pain travels with sympathetic fibres
- Pain refers T10–L1 → flank to groin
Sympathetic (T10–L1) and parasympathetic (S2–S4) fibres reach the ureter, but peristalsis is myogenic from renal pelvic pacemakers (no ureteric ganglia), and pain fibres run with sympathetics → T10–L1 dermatomes (loin to groin)
STRUCTURE & DEVELOPMENT OF URETER
1. Structure – what to actually remember
Big idea:
Ureter = muscular tube carrying urine, lined by transitional epithelium.
Histology – exam points
- Wall:
- Mainly smooth muscle + mucosa.
- Muscle:
- Under the microscope it may look like:
- Inner longitudinal
- Middle circular
- Outer longitudinal
- BUT anatomically, it’s better thought of as ONE muscular coat with fibres arranged as intertwining helices (spirals in different directions).
- This spiral arrangement helps generate peristaltic waves.
- Mucosa:
- Lined by transitional epithelium (urothelium).
- The mucosa is lax (can stretch/fold).
- No muscularis mucosae (important “negative” fact).
👉 Viva-style one-liner:
“The ureter is a smooth muscle tube with a single helical muscle coat and a lax mucosa lined by transitional epithelium, with no muscularis mucosae.”
ONE IDENTITY STATEMENT (this is the anchor)
Ureter = a smooth-muscle tube that moves urine by its own spiral muscle, lined by stretchable urothelium.
Everything else hangs from this.
🔩 Break it into ONLY what matters
① Wall composition (don’t overthink)
- Ureter wall is basically:
- Smooth muscle
- Mucosa
- No fancy gut-style layers to memorise.
🧠 Lock:
If it’s ureter → think movement, not digestion.
② Muscle layer – the BIG EXAM TRAP
What you see vs what you must think:
- Microscope may show:
- Inner longitudinal
- Middle circular
- Outer longitudinal
❗ BUT anatomically and functionally:
- It is ONE continuous muscular coat
- Fibres run as intertwining helices (spirals)
- Not clean, separate layers like intestine
🧠 Why this matters:
- Spiral fibres = wave-like squeezing
- That is how peristalsis happens
🔒 Memory lock:
“Not layers → spirals.”
If you imagine twisting a wet towel to push water down, you’ve understood the ureter.
③ Mucosa – short and deadly important
- Lined by transitional epithelium (urothelium)
- Mucosa is lax
- Can fold when empty
- Can stretch when full
- NO muscularis mucosae ❌
(this is a classic negative question)
🧠 Lock:
Ureter stretches by mucosa + muscle — not by a muscularis mucosae.
🧠 FINAL VIVA-PROOF LINE (repeat until automatic)
“The ureter is a smooth-muscle tube with a single helical muscular coat and a lax mucosa lined by transitional epithelium, with no muscularis mucosae.”
2. Development – where it comes from, and how double ureter happens
- Germ layer:
- Mesodermal origin.
- Source structure:
- Ureter develops from the ureteric bud.
- The ureteric bud sprouts from the caudal end of the mesonephric (Wolffian) duct.
- Branching of ureteric bud forms:
- Upper part divides into 2–3 branches → major calyces.
- Further branching → minor calyces.
- Further subdivision → collecting tubules/collecting ducts.
- Double ureter:
- Low division of the ureteric bud → two ureters (partial or complete duplication).
👉 So:
- Secretory part (nephrons) = metanephric tissue
- Drainage/collecting system (ureter + pelvis + calyces + collecting ducts) = ureteric bud.
🧠 THE MASTER RULE (burn this first)
Ureteric bud = DRAINAGE SYSTEM Metanephric tissue = SECRETORY SYSTEM
If you get this, all anomalies make sense.
🧬 ORIGIN — don’t scatter it
Germ layer
- Mesoderm
No ectoderm tricks. No endoderm confusion.
🌱 EXACT SOURCE (this is the exam trigger)
- Ureter develops from the ureteric bud
- Ureteric bud sprouts from the CAUDAL end of the mesonephric (Wolffian) duct
🧠 Lock image:
One tiny bud growing off the side of the Wolffian duct
🌳 WHAT THE URETERIC BUD BUILDS (drainage only)
Think branching tree 🚿
- Ureteric bud → ureter
- Upper end expands → renal pelvis
- First split → 2–3 major calyces
- Next splits → minor calyces
- Further branching → collecting ducts
🔒 Drainage rule:
If urine flows through it → it came from the ureteric bud
🧪 WHAT IT DOES NOT BUILD (secretory)
- Nephrons (glomerulus, PCT, loop, DCT)
- Come from metanephric mesenchyme (metanephric tissue)
🔒 Filtration rule:
If blood is filtered there → it came from metanephric tissue
⚠️ DOUBLE URETER — ONE SIMPLE MECHANISM
This is beautifully logical.
What goes wrong?
- Low division of the ureteric bud
What happens?
- One bud splits too early
- → Two ureteric channels
Result:
- Partial duplication (they join later)
- OR Complete duplication (two separate ureters)
🧠 Lock sentence:
Early / low split of ureteric bud = duplicated ureter
No other mechanism needed.
🧠 FINAL SKULL-STAMP (repeat this)
- Ureter is mesodermal
- Comes from ureteric bud
- Bud arises from caudal mesonephric duct
- Bud forms ureter + pelvis + calyces + collecting ducts
- Nephrons = metanephric tissue
- Low bud division = double ureter
SUPRA RENAL GLANDS
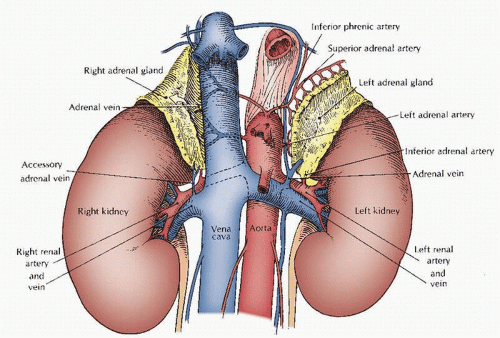
1. Big picture – what & where?
- Name: Suprarenal glands = adrenal glands (same thing).
- Position: They lie anterosuperior to the upper poles of each kidney.
- Colour & fascia:
- Yellowish endocrine glands.
- Each is in its own compartment inside the renal fascia
→ why you can remove the kidney without necessarily disturbing the gland.
👉 Mental picture: each kidney is “wearing a little yellow cap” at its upper pole, in a separate pocket of fascia.
ONE MASTER IMAGE (never change this)
Each kidney is wearing a small yellow cap — but the cap is in its own pocket.
That sentence alone answers name, position, colour, and fascia.
🔑 Break it into 3 fixed anchors
① What is it? (Name lock)
- Suprarenal gland = adrenal gland
- Two names, same structure, no trick
🧠 Lock:
“Suprarenal” just means sitting above the kidney
② Where exactly? (Position lock)
- Lies anterosuperior to the upper pole of the kidney
- Anterior (slightly in front)
- Superior (on top)
Not medial. Not posterior. Not random.
🧠 Lock:
Kidney pole → cap sits slightly forward and on top
③ Why surgery doesn’t mess it up (FASCIA = EXAM GOLD)
- Gland is:
- Yellowish (endocrine tissue look)
- Enclosed in its OWN compartment within the renal fascia
So:
- Kidney has its own fascial compartment
- Suprarenal gland has a separate fascial pocket
🧠 Clinical lock:
You can remove the kidney and leave the adrenal behind
That fact exists only because of the fascia.
🧠 FINAL VIVA SENTENCE (say this automatically)
“The suprarenal (adrenal) glands are yellowish endocrine glands lying anterosuperior to the upper poles of the kidneys, each enclosed in its own compartment within the renal fascia.”
2. Shape + key relations – RIGHT vs LEFT (very exam-friendly)
Right suprarenal gland
- Shape: Pyramidal.
- Location:
- Sits on the upper pole of the right kidney.
- Rests on the diaphragm.
- Slightly overlaps the front of the upper kidney.
- Anterior surface relations:
- Medially: overlapped by the inferior vena cava (IVC).
- Laterally/superiorly: in contact with bare area of liver.
- Inferiorly: covered by peritoneum of the posterior wall of the hepatorenal pouch.
👉 So: right gland = pyramid, between diaphragm, IVC and liver, with hepatorenal pouch peritoneum below.

Left suprarenal gland
- Shape: Crescentic (semilunar).
- Location:
- Drapes over the medial border of the left kidney above the hilum.
- Lies on the left crus of the diaphragm.
- Overlaps the front of the left kidney.
- Anterior surface relations:
- Upper part:
- Covered by peritoneum of the posterior wall of the lesser sac
- Lower part:
- In contact with body of the pancreas and splenic vessels.
→ forms part of the stomach bed.
👉 So: left gland = crescent, hugging the medial border above the hilum, related to diaphragm behind, stomach bed above, pancreas + splenic vessels below.
ONE-GLANCE MEMORY MAP (RIGHT vs LEFT)

🔺 RIGHT SUPRARENAL GLAND — THINK: “Pyramid crushed by big veins & liver”
🔑 Core lock
- Shape → Pyramidal
- Position → Upper pole of right kidney
- Posterior support → Diaphragm
👀 What touches it in front (this is what exams love)
- Medial → IVC (big, vertical, unforgiving)
- Lateral / Superior → Bare area of liver
- Inferior → Peritoneum of hepatorenal pouch (Morison pouch)
🧠 Mental picture (DO NOT skip this)
Imagine a small pyramid wedged between a giant blue IVC medially and the liver laterally, sitting on the diaphragm, with a peritoneal curtain hanging below.
📌 Reflex recall line (say this fast):
Right adrenal = pyramid + IVC medial + liver lateral + hepatorenal pouch below
🌙 LEFT SUPRARENAL GLAND — THINK: “Crescent hugging kidney, part of stomach bed”
🔑 Core lock
- Shape → Crescent / semilunar
- Position → Medial border of left kidney, above hilum
- Posterior support → Left crus of diaphragm
👀 What touches it in front (classic examiner trap)
- Upper anterior surface →
- Peritoneum of lesser sac
- → therefore part of the stomach bed
- Lower anterior surface →
- Body of pancreas
- Splenic vessels
🧠 Mental picture
See a thin crescent moon draped over the kidney’s medial edge:stomach floating in front (lesser sac above),
pancreas and splenic vessels pressing below,
diaphragm crus behind.
📌 Reflex recall line:
Left adrenal = crescent + medial kidney + stomach bed above + pancreas & splenic vessels below
⚔️ EXAM COMPARISON SNAPSHOT (LOCK THIS)
Feature | Right | Left |
Shape | Pyramidal | Crescentic |
Relation to hilum | Upper pole | Above hilum (medial border) |
Major anterior relation | IVC | Stomach (lesser sac) |
Inferior anterior relation | Hepatorenal pouch peritoneum | Pancreas + splenic vessels |
Posterior support | Diaphragm | Left crus of diaphragm |
🧩 WHY THIS NEVER GETS MIXED (logic lock)
- IVC lies on the right → only RIGHT adrenal can touch it
- Stomach + pancreas lie on the left → only LEFT adrenal relates to them
- Hence: pyramid = right, crescent = left (no exception)
🎯 FINAL EXAM-SAFE ONE-LINE (burn this in)
Right suprarenal gland is pyramidal and lies between the diaphragm posteriorly, IVC medially, liver laterally, with hepatorenal pouch peritoneum inferiorly, whereas the left suprarenal gland is crescentic, hugs the medial border above the renal hilum, lies on the left crus of the diaphragm, forms part of the stomach bed superiorly, and contacts pancreas and splenic vessels inferiorly.
BLOOD ,LYMPH,NERVE SUPPLY OF SUPRA RENAL GLAND
1. Blood supply – 3 arteries, 1 vein (and that vein matters)
Arterial supply – “3-source shower”
Each suprarenal (adrenal) gland gets rich arterial supply from three sources:
- Direct branches from the aorta
- Branches from the renal artery
- Branches from the inferior phrenic artery (usually 2–3 small branches)
👉 Big idea: very vascular glands with multiple small arteries entering the capsule.
Venous drainage – one big exit
- Despite many arteries, each gland usually has a single large vein:
- Right suprarenal vein:
- Very short – only a few millimetres.
- Drains directly into the inferior vena cava (IVC).
- Surgically dangerous – easy to tear, can cause serious bleeding.
- Left suprarenal vein:
- Longer.
- Drains into the left renal vein.
👉 What to remember for viva:
“Three arterial sources (aorta, renal, inferior phrenic), but one main vein each – short right vein to IVC, longer left vein to left renal vein.”
2. Lymph drainage – simple
- Lymph from both glands drains into para-aortic (lumbar) lymph nodes.
(That matches kidney & upper ureter drainage pattern.)
🧠 SUPRARENAL GLAND — BLOOD, LYMPH, NERVE
(Think: MANY ways in, ONE risky way out)
🔴 1. BLOOD SUPPLY — “3 arteries shower, 1 vein escape”
🩸 Arteries — 3-source shower 🚿
Each suprarenal gland is extremely vascular.
Three arterial sources (remember: A–R–P):
- Aorta → middle suprarenal arteries
- Renal artery → inferior suprarenal artery
- Inferior phrenic artery → superior suprarenal arteries(highest)
- usually 2–3 small branches
👉 Mental picture:
The gland is being sprayed from above, side, and below.
EXAM LINE:
“Suprarenal glands receive a rich arterial supply from aorta, renal artery, and inferior phrenic artery.”
🔵 Veins — ONE big exit (THIS IS THE TRAP ⚠️)
Despite many arteries → ONLY ONE main vein per gland.
➡️ Right suprarenal vein ⚠️
- Very short
- Drains directly into IVC
- High surgical risk → tears easily → massive bleeding
⬅️ Left suprarenal vein
- Longer
- Drains into left renal vein (safer)
👉 Memory lock 🔐:
“Right = short + straight to IVC = dangerous”
“Left = longer + joins renal vein = safer”
VIVA ONE-LINER:
“Each suprarenal gland has a single vein — right drains directly to IVC, left drains to left renal vein.”
🟢 2. LYMPH DRAINAGE — Follow the artery rule
- Lymph from both suprarenal glands → para-aortic (lumbar) lymph nodes
👉 Same logic as:
- Kidney
- Upper ureter
MEMORY HOOK:
“Upper retroperitoneal organs → para-aortic nodes”
🟡 3. NERVE SUPPLY — Hormone release is neural-driven
(This is often forgotten — examiners LOVE it)
🔌 Sympathetic supply (KEY)
- Preganglionic sympathetic fibres
- Origin: T10–L1
- Travel via:
- Greater splanchnic nerves
- Synapse DIRECTLY on chromaffin cells
👉 Critical concept:
The adrenal medulla behaves like a modified sympathetic ganglion.
Result:
- Direct release of adrenaline & noradrenaline into blood
❌ Parasympathetic
- No significant parasympathetic supply
🧠 FINAL MEMORY BLOCK (EXAM-READY)
- Arteries: 3 sources → Aorta + Renal + Inferior phrenic
- Veins: 1 vein each
- Right → short → IVC (dangerous)
- Left → long → left renal vein
- Lymph: → Para-aortic nodes
- Nerves:
- Preganglionic sympathetic (T10–L1)
- Medulla = modified sympathetic ganglion
3. Nerve supply – medulla vs cortex logic
Medulla – like a modified sympathetic ganglion
- Main nerve supply:
- Myelinated preganglionic sympathetic fibres.
- Come via splanchnic nerves → coeliac plexus → into gland.
- These preganglionic fibres synapse directly on medullary cells.
- Medullary cells = modified postganglionic sympathetic neurons.
- They release adrenaline & noradrenaline into blood.
- Blood vessels in the gland:
- Get usual postganglionic sympathetic fibres for vasomotor tone.
👉 Exam phrase:
“Adrenal medulla receives preganglionic sympathetic fibres that synapse directly on medullary cells – a modified sympathetic ganglion.”
Cortex – no direct nerve control
- Cortex is not controlled neurally.
- Its activity is regulated by hormones, especially:
- ACTH from anterior pituitary → controls cortisol & androgens secretion.
👉 Key contrast:
- Medulla: neural control via sympathetic preganglionic fibres.
- Cortex: mainly humoral control via ACTH, not nerves.
🧠 ONE CORE PICTURE (build this first)
Imagine the adrenal gland as TWO ORGANS stuck together:
- Inside = MEDULLA → behaves like a SYMPATHETIC GANGLION
- Outside = CORTEX → behaves like an ENDOCRINE GLAND
If you hold this picture, everything else becomes automatic.
🔥 MEDULLA = “NERVOUS SYSTEM ORGAN”
Think: sympathetic ganglion without axons
- Input:
- Myelinated preganglionic sympathetic fibres
- Path: splanchnic nerves → coeliac plexus → adrenal medulla
- Synapse:
- Directly on chromaffin (medullary) cells
- What are chromaffin cells?
- Modified postganglionic sympathetic neurons
- Output:
- Adrenaline + noradrenaline
- Released straight into bloodstream (no synaptic cleft)
👉 Why special?
Normal sympathetic pathway = 2 neurons
Adrenal medulla = only 1 neuron (preganglionic)
⚡ Exam reflex line
“Adrenal medulla is a modified sympathetic ganglion receiving preganglionic fibres.”
🧊 CORTEX = “HORMONE-ONLY ORGAN”
Think: no nerves allowed inside
- NO direct neural control
- Regulated by humoral signals
- Main controller:
- ACTH (anterior pituitary) → cortisol + adrenal androgens
- Aldosterone mainly via:
- RAAS + potassium (not nerves)
👉 Even if nerves pass nearby → they do NOT control secretion
⚠️ Common exam trap
❌ “Sympathetic nerves stimulate adrenal cortex” → FALSE
🩸 VESSELS (tie the loose end)
- Blood vessels of the gland:
- Do receive postganglionic sympathetic fibres
- Purpose = vasomotor control only
- NOT hormone secretion
🔒 FINAL EXAM LOCK (repeat this)
- Medulla → Neural, preganglionic sympathetic, modified ganglion
- Cortex → Hormonal, ACTH/RAAS, no neural control
- Vessels → sympathetic only for blood flow
STRUCTURE OF SUPRARENAL GLAND
1. Big picture – cortex vs medulla
- Suprarenal (adrenal) gland has:
- Outer yellow cortex – thick.
- Inner grey medulla – thinner, in the centre.
- Cortex completely surrounds the medulla.
👉 Exam idea: two different structure, function, and embryological origins.
2. Cortex – 3 zones, 3 main hormone groups
Cortex produces mainly:
- Cortisol (glucocorticoid)
- Aldosterone (mineralocorticoid)
- Androgens (sex steroids) + related hormones
Histologically, it has 3 zones (outside → inside):
- Zona glomerulosa
- Just under the capsule.
- Small rounded cells in clusters.
- Main product (functionally): mineralocorticoids → aldosterone.
- Zona fasciculata
- Thickest zone.
- Parallel cords (“fascicles”) of pale, vacuolated cells (lipid-rich).
- Main product: glucocorticoids → cortisol.
- Zona reticularis
- Innermost cortical layer, close to medulla.
- Network (“reticulum”) of smaller, darker cells.
- Main product: androgens (and related steroids).
Classic memory:
“G–F–R = Salt, Sugar, Sex” (super exam-friendly):
- Glomerulosa → Salt (aldosterone, Na⁺ balance)
- Fasciculata → Sugar (cortisol, glucose metabolism)
- Reticularis → Sex (androgens)
3. Medulla – catecholamine factory + chromaffin reaction
- Medulla is relatively small and central.
- Its cells secrete catecholamines:
- About 80% adrenaline (epinephrine)
- About 20% noradrenaline (norepinephrine)
- Plus some dopamine
Chromaffin reaction:
- Many medullary cells contain fine granules (catecholamine precursors).
- These granules are stained brown by chromium salts → “chromaffin” cells.
- This is why the adrenal medulla is described as a chromaffin tissue.
Blood:
- Dilated capillaries are prominent in the medulla, not so much in the cortex.
→ fits with medulla’s role of releasing hormones directly into blood quickly.
4. Development – dual origin (very high-yield)
- Medulla:
- Derived from neural crest cells.
- So it is ectodermal in origin.
- Fits its role as a modified sympathetic ganglion (SNS-like cells).
- Cortex:
- Develops in situ from mesoderm.
- Specifically from intermediate cell mass (intermediate mesoderm).
👉 Exam sentence to memorise:
“Adrenal medulla is ectodermal (neural crest); adrenal cortex is mesodermal (intermediate cell mass).”
ONE CORE MENTAL MODEL (this does the work)
Build the adrenal gland in two steps:
- First, a mesodermal shell forms in the embryo
- Later, neural crest cells migrate into it
That’s it.
If you remember migration, the origins never flip.
🧊 CORTEX = “FORMED IN PLACE” (MESODERM)
- Develops in situ
- Origin: Intermediate mesoderm
- Behaves like a classic endocrine gland
- Secretes steroids (cortisol, aldosterone, androgens)
🧠 Memory hook
“Steroids come from mesoderm.”
🔥 MEDULLA = “MIGRANT CELLS” (ECTODERM)
- Derived from neural crest cells
- Neural crest = ectoderm
- Cells migrate into the developing cortex
- Become chromaffin cells
- Function as modified sympathetic neurons
🧠 Memory hook
“Neural crest always migrates → medulla must be ectoderm.”
🔁 LOGIC LOOP (repeat mentally)
- Neural crest → ectoderm → medulla → catecholamines
- Intermediate mesoderm → cortex → steroids
Once this loop is stable, MCQs become reflex.
🔒 ONE-LINE EXAM LOCK (don’t change wording)
“Adrenal medulla is ectodermal in origin from neural crest cells, while adrenal cortex is mesodermal from the intermediate cell mass.”
SURGICAL APPROACH
1. Main approaches – when do you use which?
a) Bilateral adrenalectomy (both glands)
- Approach:
- Usually anterior, transperitoneal, via a bilateral subcostal “rooftop” incision.
- Same route used for laparoscopic bilateral adrenalectomy (just with ports, not a big open cut).
👉 So: both glands = front, rooftop, transperitoneal.
b) Unilateral adrenalectomy (one gland, e.g. tumour)
- Approach:
- Posterolateral, extraperitoneal, through the bed of the 12th rib.
- For large adrenal tumour:
- May need a higher approach → via 11th or 10th rib bed.
- Sometimes requires division of the diaphragm to get enough exposure.
👉 So: one gland = back/side, extraperitoneal via 12th rib; big tumour = higher (11th/10th), may cut diaphragm.
2. How they reach EACH gland in the anterior (rooftop) approach
Right adrenal gland
- After opening abdomen with rooftop incision:
- Right lobe of liver is retracted upwards.
- A Kocher manoeuvre is done:
- Mobilizes the second part of duodenum + head of pancreas.
- These are reflected and lifted off the upper pole of the right kidney and IVC.
- This exposes:
- Right suprarenal gland
- Upper kidney
- Inferior vena cava (very close!).
Left adrenal gland
- Steps:
- Phrenicocolic ligament is divided → allows splenic flexure of colon to be mobilized downward.
- Posterior layer of the splenorenal ligament is incised.
- Spleen + tail of pancreas are turned medially.
- This exposes:
- Left suprarenal gland
- Upper part of left kidney
👉 Key idea:
- Right: liver up + Kocher manoeuvre (duodenum & pancreas mobilized).
- Left: mobilize splenic flexure → open splenorenal ligament → spleen + pancreas tail medially.
3. Vein first, then arteries – and why the right side is risky
- On both sides:
- Suprarenal vein is ligated BEFORE the many small arteries.
Why?
- To stop the gland dumping large amounts of hormones (especially catecholamines) into the circulation during handling.
- Therefore: handle gland as little as possible before venous ligation.
Right suprarenal vein:
- Very short, goes directly into IVC.
- IVC is easily torn if the vein is pulled or mishandled.
- So right side is technically more dangerous from a vascular standpoint.