⭐ LUMBAR PLEXUS
(L1–L4; inside psoas major)
Major function: Motor + sensory to anterior thigh, medial thigh, inguinal region, and parts of abdominal wall.
🔥 SUPER-HIGH YIELD — 5 NERVES YOU MUST KNOW
1. Iliohypogastric & Ilioinguinal (L1)
What to remember (exam gold):
- Not really part of plexus → continuation of segmental body-wall nerves,
- Motor: Internal oblique + transversus abdominis (roof of inguinal canal).
- Sensory: Skin of inguinal region + anterior scrotum/labia.
Course in relation to psoas
- Both nerves arise from L1 →
- Emerge from the lateral border of psoas major →
- Cross obliquely over the anterior surface of quadratus lumborum →
- Then pierce transversus abdominis near the iliac crest.
Clinicals:
- Injury → loss of sensation over groin + weakened inguinal canal → predisposition to inguinal hernia.
Clinical scinario
A 38-year-old man comes to surgical clinic 10 days after an open appendicectomy done through a right lower abdominal (gridiron/Lanz) incision. He says:
- “Doctor, my right groin is numb… like a patch of skin doesn’t feel normal.”
- “Also the front part of my scrotum feels dull.”
- Since the operation he also notices a new bulge in the right groin that appears when he coughs or strains and reduces when he lies down.
On exam you find:
1) The “exam-gold” nerve story
During the incision and muscle splitting, a segmental body-wall nerve from L1 was likely injured — not truly a ‘classic plexus’ nerve, but more a continuation of the segmental body-wall nerve pattern.
The two likely nerves are:
- Iliohypogastric (L1)
- Ilioinguinal (L1)
2) Why his symptoms match L1 iliohypogastric/ilioinguinal
Sensory findings (very typical):
- Reduced sensation in the inguinal region skin (groin)
- Reduced sensation over the anterior scrotum (or labia in females)
That directly matches the sensory supply you listed.
3) Why a hernia can appear after this injury (the “mechanism”)
He also has a cough-impulse groin bulge → suggests an inguinal hernia tendency because these nerves give motor supply to key abdominal wall muscles:
- Internal oblique
- Transversus abdominis
These muscles form the roof of the inguinal canal and contribute to the dynamic “shutter” protection of the canal.
So if the iliohypogastric/ilioinguinal nerves are injured:
- internal oblique + transversus abdominis become weaker/denervated in that area
→ roof support weakens
→ posterior wall/roof protection reduces during raised intra-abdominal pressure
→ predisposition to inguinal hernia (especially post-op when coughing/straining).
4) “Course in relation to psoas” explained inside the scenario (so you can narrate it in viva)
When the surgeon worked in the lateral abdominal wall plane, these nerves were in the danger zone because:
- Both arise from L1
- They emerge from the lateral border of psoas major
- Then they run obliquely across the anterior surface of quadratus lumborum
- Then they pierce transversus abdominis near the iliac crest
That path puts them exactly where lower abdominal incisions and muscle splitting can catch them — especially around the flank/iliac crest region and in the internal oblique/transversus plane.
5) Finish the case with the “exam conclusion”
So the unified diagnosis line you’d say is:
“Post-operative injury to L1 segmental body-wall nerves — iliohypogastric and/or ilioinguinal — causing groin + anterior scrotal/labial sensory loss, plus denervation of internal oblique and transversus abdominis weakening the roof of the inguinal canal, predisposing to an inguinal hernia.”
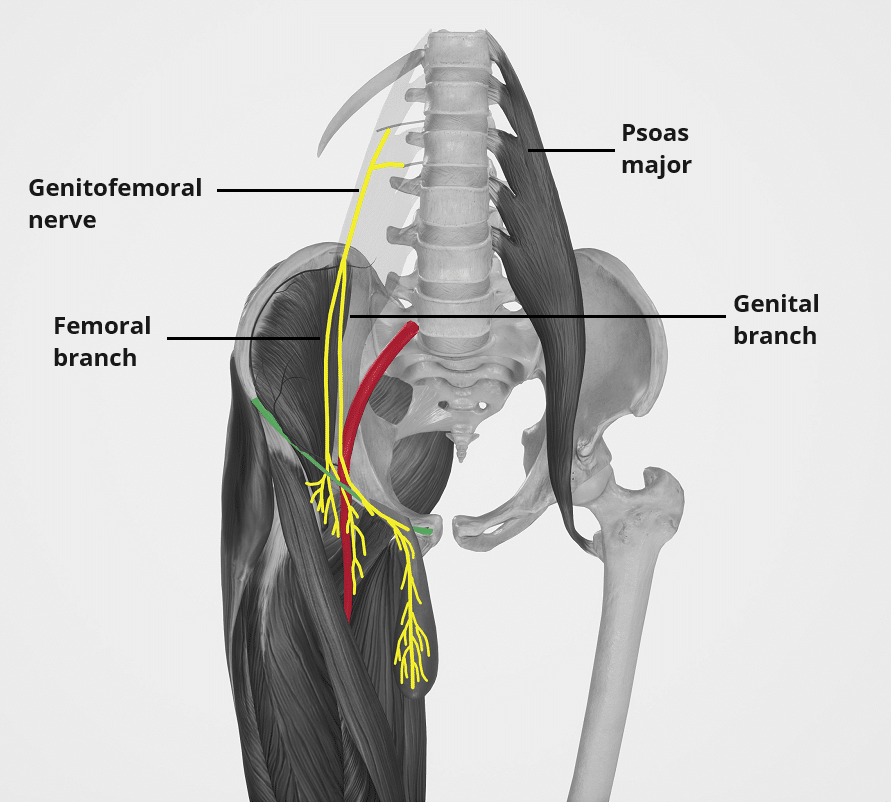
2. Genitofemoral (L1–L2)
Key exam points:
Divides into Genital + Femoral branches:
- Genital branch:
- Sensory → spermatic fascia, tunica vaginalis.
- Motor → cremaster muscle (→ cremasteric reflex).
- Femoral branch:
- Sensory → skin below middle inguinal ligament.
COURSE
1️⃣ Emergence
- Formed within the psoas major.
- Pierces the anterior surface of psoas major (THIS is the key landmark).
2️⃣ Descent
- Runs down the anterior surface of psoas major, vertically.
- Descends towards the inguinal ligament.
3️⃣ Division (very high yield)
- Divides above the inguinal ligament into:
- Genital branch
- Femoral branch
4️⃣ Final Courses
Genital branch
- Runs through the deep inguinal ring → inguinal canal
- Ends in:
- Cremaster muscle (motor)
- Scrotal/labial skin (sensory)
Femoral branch
- Passes beneath inguinal ligament
- Enters femoral sheath (lateral compartment)
- Supplies skin below the inguinal ligament.
Clinicals:
- Cremaster reflex absent in testicular torsion.
Integrated Clinical Scenario – Genitofemoral Nerve (L1–L2)
A 22-year-old male presents to the emergency department with sudden onset severe left scrotal pain radiating to the groin and lower abdomen. The pain started abruptly while he was resting. He feels nauseated and is unable to find a comfortable position.
Step 1: Initial Examination (linking sensory anatomy)
On inspection, the left testis is high-riding. Palpation reveals marked tenderness. When the clinician lightly strokes the inner aspect of the left thigh, there is no elevation of the left testis.
👉 This immediately suggests loss of the cremasteric reflex.
Step 2: Explaining the Missing Cremasteric Reflex (motor pathway)
- The cremasteric reflex depends on the genital branch of the genitofemoral nerve (L1–L2).
- The genital branch provides:
- Motor supply to the cremaster muscle
- Sensory supply to spermatic fascia and tunica vaginalis
In this patient:
- Testicular torsion twists the spermatic cord
- This compromises the genital branch of the genitofemoral nerve
- Result → cremaster muscle cannot contract
- Hence → absent cremasteric reflex
This is why absence of the cremasteric reflex is a classic clinical sign of testicular torsion.
Step 3: Tracing the Nerve Course to the Pathology (course = exam gold)
Understanding the course explains why this nerve is affected:
- Formation within psoas major (L1–L2)
- Pierces the anterior surface of psoas major
- Runs vertically down the anterior surface of psoas
- Divides above the inguinal ligament into:
- Genital branch
- Femoral branch
→ key landmark distinguishing it from ilioinguinal/iliohypogastric nerves
The genital branch:
- Enters the deep inguinal ring
- Traverses the inguinal canal
- Supplies:
- Cremaster muscle (motor)
- Scrotal/labial skin & tunica vaginalis (sensory)
Because the torsion occurs within the inguinal canal/spermatic cord, the genital branch is directly compromised.
Step 4: Differentiating from Other Causes Using Femoral Branch Anatomy
On sensory testing:
- The patient also reports normal sensation over skin below the middle of the inguinal ligament.
Why?
- The femoral branch of the genitofemoral nerve:
- Passes beneath the inguinal ligament
- Enters the femoral sheath (lateral compartment)
- Supplies skin below the middle of the inguinal ligament
Since torsion affects the inguinal canal, the femoral branch remains intact, helping localize the lesion specifically to the genital branch.
Step 5: Clinical Correlation & Surgical Importance
- During inguinal hernia repair, orchidopexy, or laparoscopic pelvic surgery, the genitofemoral nerve is at risk because it:
- Lies on the anterior surface of psoas major
- Divides just above the inguinal ligament
Iatrogenic injury can cause:
- Loss of cremasteric reflex
- Scrotal or labial numbness
- Chronic groin pain
Final Integrated Take-Home (exam-ready)
- Absent cremasteric reflex → think genital branch of genitofemoral nerve
- Genitofemoral nerve hallmark → pierces anterior surface of psoas major
- Division above inguinal ligament is very high-yield
- Testicular torsion classically abolishes the reflex due to genital branch compromise
- Femoral branch supplies skin below the inguinal ligament and is spared in torsion
This single scenario ties together origin, course, branches, motor and sensory supply, and clinical relevance — exactly how examiners expect it.
3. Lateral Femoral Cutaneous (L2–L3, posterior divisions)
Must-know:
- Pure sensory nerve.
- Lateral thigh down to knee.
- Passes under or through lateral inguinal ligament.
1️⃣ ORIGIN
- Comes from posterior divisions of L2–L3.
- Arises from the lateral border of psoas major.
2️⃣ COURSE (VERY HIGH YIELD)
A. Across Iliacus
- After emerging from the lateral border of psoas major →It runs obliquely across the iliacus muscle.
- Deep to the iliac fascia (exam gold line).
B. Towards the ASIS
- Travels toward the anterior superior iliac spine (ASIS).
- Key landmark: Nerve passes near or through the inguinal ligament.
C. Passage under the Inguinal Ligament
- It passes beneath the inguinal ligament, usually:
- Medial to the ASIS (MOST common path),
- Sometimes through the ligament
- Rarely lateral to ASIS (compression risk ↑ in this variant).
3️⃣ DISTRIBUTION (Sensory-only)
- Purely sensory nerve.
- Supplies:
- Skin on the lateral thigh
- From hip → knee
No motor supply. No reflexes associated.
4️⃣ CLINICALS (EXTREMELY HIGH YIELD)
Meralgia Paresthetica
Compression of this nerve →
🔸 Burning pain
🔸 Numbness
🔸 Tingling
🔸 On lateral thigh
Risk factors:
- Tight belts
- Tight jeans
- Pregnancy
- Obesity
- Prolonged standing
Worst compression point:
➡️ Where nerve passes under the inguinal ligament.
Clinical:
- Entrapment → Meralgia Paresthetica (burning, numbness lateral thigh).
A 38-year-old man comes to clinic with a very specific complaint: for 3 weeks he has had a burning, tingling “electric” discomfort over the outer side of his right thigh, starting near the front of the hip and running down toward the knee. He says it feels like the skin is “on fire” and sometimes becomes numb. He keeps rubbing the area and says, “It’s only the skin—my muscles feel normal.”
History that quietly gives the diagnosis
- He recently started a new security job with prolonged standing.
- He also began wearing a tight leather belt to carry equipment, and sometimes tight jeans under the uniform.
- He has gained weight in the past year (obesity risk factor).
- Pain is worse after long standing/walking and when the belt is tight, and improves when he loosens the belt or sits.
- He denies back pain radiating down the leg, and there is no weakness.
Examination (the examiners’ “trap-rescue” moment)
- Motor power is normal in hip flexion/extension, knee extension, ankle movements.
- Reflexes are normal (no reflex involvement).
- On sensory testing, there is reduced sensation and dysesthesia over the lateral thigh skin (hip → knee region).
- No tenderness along the lumbar spine, and straight-leg raise does not reproduce symptoms (helps separate from radiculopathy).
- When you palpate just medial to the ASIS and press along the line of the inguinal ligament, he jumps and says, “That’s the exact spot it shoots from.”
→ This is the classic entrapment point.
What is happening anatomically (linked to your lines, step-by-step)
This is meralgia paresthetica due to compression of the lateral femoral cutaneous nerve:
- Origin
- Nerve is from posterior divisions of L2–L3.
- It emerges from the lateral border of psoas major.
- Course (the reason it gets trapped)
- After leaving psoas, it runs obliquely across iliacus.
- It lies deep to the iliac fascia (your “exam gold line”).
- It heads toward the ASIS.
- Then it approaches the inguinal ligament and usually passes beneath the inguinal ligament, most commonly medial to the ASIS.
- Sometimes it goes through the ligament.
- Rarely it passes lateral to ASIS (that variant makes compression risk higher).
- Distribution
- It is pure sensory → supplies skin of the lateral thigh from hip to knee.
- That’s why:
- Burning pain / tingling / numbness are present,
- BUT no motor deficit and no reflex change.
Why his risk factors matter (mechanism)
The nerve is “pinched” where it is forced to pass a tight corner under/through the inguinal ligament near the ASIS:
- Tight belt / tight jeans → direct external compression at the inguinal ligament.
- Obesity → increased pressure and tension across the inguinal ligament region.
- Pregnancy (classic) → increased abdominal mass and pelvic tilt increases stretch/compression.
- Prolonged standing → sustained tension across that region.
How you’d summarize to the examiner in one clean sentence
“Pure sensory L2–L3 nerve, emerges lateral to psoas, crosses iliacus deep to iliac fascia, passes near ASIS under/through inguinal ligament—compression there causes meralgia paresthetica with lateral-thigh burning/tingling/numbness and no motor or reflex loss.”
4. Femoral Nerve (L2–L4 posterior divisions) — MOST IMPORTANT
REMEMBER 3 THINGS:
- Course:
- Lateral border of psoas → crosses iliacus → under inguinal ligament → femoral triangle.
- Motor:
- Quadriceps (knee extension).
- Iliacus, sartorius, pectineus.
- Sensory:
- Anterior thigh + medial leg (via saphenous nerve).
Clinicals:
- Femoral nerve injury →
- Loss of knee extension
- Absent patellar reflex
- Sensory loss: anterior thigh + medial leg.
Elaborative clinical scenario — Femoral nerve (L2–L4) injury (everything connected)
A 42-year-old man comes to the emergency unit after a road-traffic accident. He had a deep groin laceration and a big painful swelling just below the inguinal ligament region. In theatre, surgeons control bleeding near the femoral triangle area.
After surgery, once he wakes up, he complains:
- “Doc, my leg is weak… I can’t straighten my knee.”
- “When I try to walk, my knee feels like it will buckle.”
- “Also there’s numbness in front of my thigh and along the inner side of my leg.”
1) Why this pattern happens — tie it to the COURSE (exam scoring)
On examination, the team suspects femoral nerve injury because the injury site is exactly where the femoral nerve travels:
- The femoral nerve forms from L2–L4 posterior divisions in the pelvis.
- It emerges from the lateral border of psoas major.
- Then it runs across the iliacus muscle (in the iliac fossa).
- Then it passes under the inguinal ligament.
- Immediately after that, it enters the femoral triangle, where it is vulnerable during:
- penetrating trauma,
- groin/femoral triangle surgery,
- procedures around the inguinal ligament region.
So a cut/traction/compression in that zone can damage the femoral nerve right before/within the femoral triangle.
2) What you see on MOTOR exam — connect to muscles
Main functional complaint
When asked to extend his knee against resistance, he cannot.
That happens because femoral nerve supplies the:
- Quadriceps femoris → knee extension (the most important motor job).
So clinically you see:
- Difficulty rising from a chair
- Difficulty climbing stairs
- “Knee giving way” while walking (because quadriceps normally stabilizes the knee in stance phase)
Other motor losses you can demonstrate
Because the femoral nerve also supplies:
- Iliacus → hip flexion weakness (hip flexion is not completely lost because other hip flexors still work, but it becomes weaker)
- Sartorius → contributes to hip flexion and positioning movements (patient may feel clumsy bringing leg into certain positions)
- Pectineus (often femoral nerve contribution) → mild weakness in hip flexion/adduction components
So on exam you’ll often find:
- Weak hip flexion (partial)
- Marked weak/absent knee extension (biggest sign)
3) Reflex finding — the “instant diagnosis” clue
You test the patellar reflex (knee jerk):
- It is absent on the affected side.
Why?
- Patellar reflex = quadriceps reflex arc
- Femoral nerve carries both the sensory + motor limbs of that reflex
So:
- Femoral nerve injury → absent patellar reflex (classic, high-yield)
4) Sensory map — connect to the saphenous nerve
Pinprick/light touch testing shows:
- Reduced sensation over the anterior thigh (femoral cutaneous territory)
- Reduced sensation along the medial leg down towards the medial side of the lower limb — because of the saphenous nerve, which is:
- a sensory branch of the femoral nerve
- responsible for medial leg sensation
So the patient’s line:
“front of thigh numb + inner side of leg numb”matches exactly:
- Anterior thigh + medial leg (via saphenous nerve)
Wrap-up: One clean diagnosis statement
Because the injury is near the inguinal ligament/femoral triangle, and the patient has:
- Loss of knee extension (quadriceps)
- Absent patellar reflex
- Sensory loss: anterior thigh + medial leg (saphenous)
→ This is a classic femoral nerve (L2–L4) injury.
5. Obturator Nerve (L2–L4 anterior divisions)
Key points:
- From medial side of psoas → through obturator canal → splits into anterior & posterior divisions.
Course / Pathway
- In pelvis
- Forms within psoas major.
- Emerges from its medial border.
- Runs along lateral wall of pelvis:
- On obturator internus muscle
- With obturator artery & vein.
- Reaches obturator canal (upper part of obturator foramen).
- Through obturator canal
- Enters thigh via obturator canal.
- Here it usually divides into:
- Anterior division
- Posterior division
- In the thigh
- Anterior division:
- Lies between adductor longus (superficial) and adductor brevis (deep).
- Posterior division:
- Passes through or behind obturator externus, then
- Runs on anterior surface of adductor magnus, deep to adductor brevis.
- supply knee
Motor Supply (Muscles)
Main nerve of the medial (adductor) compartment of thigh:
- Obturator externus
- Adductor longus
- Adductor brevis
- Adductor part of adductor magnus
- Gracilis
- Sometimes a twig to pectineus (more often from femoral but can be shared).
Roughly:
- Anterior division:
- Adductor longus
- Adductor brevis
- Gracilis
- Posterior division:
- Obturator externus
- Adductor magnus (adductor part)
Sensory Supply
- Articular branches:
- To hip joint (from anterior division).
- To knee joint (from posterior division – travels with the branch to the knee, often via the popliteal fossa).
- Cutaneous:
- Variable cutaneous branch to medial thigh skin (mid-portion).
Clinical scinario
A 34-year-old man comes after a pelvic lymph node dissection / obturator node clearance (or after fixation of an acetabular + superior pubic ramus fracture). Since surgery he says:
- “Inner thigh numb and burning… and I can’t pull my legs together properly.”
- He also gets deep groin pain when he tries to walk fast or climb stairs, and a dull ache near the medial knee that feels “inside the joint.”
On exam, you build the whole story directly from the obturator nerve’s pathway + its anterior/posterior divisions:
1) Why this surgery/fracture can hit the obturator nerve (pelvic course)
During pelvic surgery, the nerve is vulnerable exactly where it normally runs:
- The obturator nerve forms within psoas major (L2–L4 anterior divisions).
- It then emerges from the medial border of psoas.
- From there it runs along the lateral wall of the pelvis, lying on obturator internus, and it travels with the obturator artery and vein.
- It heads to the obturator canal (the upper part of the obturator foramen).
So, in an obturator node dissection / pelvic side-wall work, or with bleeding/hematoma along that side-wall, you can get:
- direct traction injury,
- compression by hematoma,
- or entrapment/scarring near the obturator canal.
2) The “obturator canal moment” explains the mixed deficits
As the nerve passes through the obturator canal, it enters the thigh and usually divides right there into:
- Anterior division
- Posterior division
So the patient’s symptoms can be:
- pure obturator (both divisions affected), or
- selective (one division more affected), depending on where the lesion is (pelvis vs canal vs thigh).
3) Thigh findings that map perfectly to anterior vs posterior division course
A) Anterior division course → explains adductor weakness + medial thigh sensory issues
In the thigh the anterior division normally lies:
- between adductor longus (superficial) and adductor brevis (deep).
So if the lesion affects this division, you see:
Motor (anterior division muscles):
- Adductor longus
- Adductor brevis
- Gracilis
Bedside functional sign:
- Weakness of hip adduction → difficulty bringing thighs together (trouble stabilizing pelvis while walking; feels “wobbly” on direction changes).
Sensory (cutaneous branch):
- A variable cutaneous area of altered sensation over the mid-medial thigh skin.
- Key exam trick: it’s often patchy/variable because the cutaneous branch is variable.
That matches his complaint: burning/numbness in mid medial thigh + can’t adduct well.
B) Posterior division course → explains deep weakness + knee symptoms
The posterior division normally:
- passes through or behind obturator externus, then
- runs on the anterior surface of adductor magnus, deep to adductor brevis
- and importantly gives an articular branch to the knee.
So involvement here produces:
Motor (posterior division muscles):
- Obturator externus
- Adductor part of adductor magnus
Clinical feel:
- Less obvious “surface” weakness than anterior division injury, but there’s still loss of strong, sustained adduction (especially powerful adduction work).
Knee joint complaint (posterior division articular branch):
- Referred ache “inside” the knee joint, sometimes felt towards the popliteal region because the knee articular branch can track with the branch toward the knee (classically described as potentially reaching via the route that can be perceived near the back of the knee).
- Exam clue: knee pain without primary knee pathology signs.
That matches his: medial knee joint ache despite a normal knee exam.
4) Hip joint pain is explained too (anterior division articular branch)
You also explain his deep groin pain:
- The hip joint articular branch comes from the anterior division.
So an obturator nerve lesion can present with:
- deep hip/groin pain (joint-like), especially on hip movement or weight-bearing,
- even if the hip muscles themselves look okay.
That’s why he feels groin pain on stairs/walking fast.
5) Full “medial compartment motor” pattern (what you test and what you find)
When you test the classic obturator-innervated medial compartment group, you intentionally cover every muscle you listed:
Main motor supply (medial thigh):
- Obturator externus
- Adductor longus
- Adductor brevis
- Adductor part of adductor magnus
- Gracilis
- ± Pectineus twig sometimes (often femoral, but may be shared)
Exam maneuvers:
- Ask him to adduct thighs against resistance (squeeze your fist or a pillow between knees).
- Weakness is obvious if anterior division is involved (longus/brevis/gracilis).
- Power loss can persist if posterior division involved (magnus adductor part + obturator externus).
- Gait: he may have a subtle wide-based/unstable gait because adductors help stabilize pelvis and control limb swing.
6) Put it together as a single clean diagnosis statement
So you conclude:
“This is an obturator nerve injury at/near the obturator canal or pelvic side-wall.”
Because the case has:
- motor adductor weakness (medial compartment pattern),
- variable medial thigh cutaneous sensory change
- hip joint pain (anterior division articular),
- knee joint pain (posterior division articular),
- formation in psoas, emergence medial border, course on obturator internus with obturator vessels, passage through obturator canal, and division into anterior/posterior with their specific thigh planes and targets.
all of which map exactly to:
⭐ SUPER-SUMMARY TABLE (MEMORY HACK)
Nerve | Roots | Sensory | Motor | Key Clinical |
Iliohypogastric | L1 | Suprapubic | Internal oblique, TA | Weak inguinal canal |
Ilioinguinal | L1 | Groin, scrotum/labia | Same muscles | Hernia risk |
Genitofemoral | L1–L2 | Scrotum/labia, skin below IL | Cremaster | Cremaster reflex |
Lat. Fem. Cutaneous | L2–L3 | Lateral thigh | None | Meralgia paresthetica |
Femoral | L2–L4 | Anterior thigh, medial leg | Quadriceps, iliacus, sartorius | Loss knee extension |
Obturator | L2–L4 | Medial thigh | Adductors | Loss adduction |
⭐ SACRAL PLEXUS
(L4–S4, on anterior surface of piriformis)
Main functions:
- Motor: Posterior thigh, all of leg & foot, gluteal muscles, pelvic floor, perineum
- Sensory: Posterior thigh, leg, foot, perineum, penis/clitoris, buttock skin
- Autonomic: Parasympathetic to pelvic organs
🔥 THE 6 NERVES YOU MUST KNOW
1. SCIATIC NERVE — THE KING 👑
Roots: L4–S3
Largest nerve in the body.
Motor:
- ALL hamstrings (except short head of biceps — common peroneal)
- ALL muscles of leg & foot (via tibial + common peroneal)
Sensory:
- MOST of leg and foot (via branches)
Course (super high yield):
- Leaves pelvis below piriformis
- Between greater trochanter & ischial tuberosity
- Runs down posterior thigh → splits to tibial + common peroneal
Clinical GOLD:
- Piriformis syndrome
- Sciatica
- Foot drop (common peroneal part)
- Hamstring weakness
2. PUDENDAL NERVE — NERVE OF PERINEUM 🚻
1. Origin & Root Value
- Roots: S2, S3, S4 (ventral rami – anterior divisions).
- Part of the sacral plexus.
- Classic line: “S2–S4 keep the pelvic floor off the floor” – pudendal is the main somatic nerve for perineum.
2. Nature of the Nerve
- Type: Somatic mixed nerve
- Motor: Striated muscles of perineum & external sphincters.
- Sensory: Skin of perineum & external genitalia.
- NOT autonomic, but:
- Travels close to pelvic splanchnic nerves (S2–S4) and pelvic plexus, which carry parasympathetic fibres for pelvic organs.
3. Course (Stepwise – very exam-y)
- In pelvis
- Arises from S2–S4 ventral rami in the sacral plexus.
- Lies on the anterior surface of piriformis and sacrospinous ligament region.
- Medial to the ischial spine initially.
- Exits pelvis
- Leaves pelvis through the greater sciatic foramen, below piriformis.
- Runs medial to sciatic nerve and posterior to ischial spine & sacrospinous ligament.
- Hook around ischial spine
- Curves around the ischial spine and sacrospinous ligament (this is the landmark for pudendal nerve block).
- Re-enters pelvic/perineal region
- Enters perineum through the lesser sciatic foramen.
- Now lies in the ischioanal fossa.
- In pudendal canal (Alcock’s canal)
- Runs forward in the pudendal canal:
- A fascial tunnel in the obturator internus fascia on lateral wall of ischioanal fossa.
- Accompanied by internal pudendal vessels (artery & vein).
- Terminal distribution
- Within/just beyond the canal it divides into its three main terminal branches.
4. Branches (Main Named Branches)
1️⃣ Inferior rectal (anal) nerves
- Usually arise near the posterior part of the ischioanal fossa (often from pudendal nerve in the canal, sometimes directly from S4).
- Course:
- Cross the fat of ischioanal fossa medially to the anal canal.
- Supply:
- Motor: External anal sphincter.
- Sensory: Lower half of anal canal (below pectinate line) + perianal skin.
2️⃣ Perineal nerve
Divides into deep (motor) and superficial (sensory) branches.
- Deep perineal branches (motor):
- Supply perineal muscles, e.g.:
- Superficial & deep transverse perineal muscles
- Bulbospongiosus
- Ischiocavernosus
- External urethral sphincter (via branches in deep perineal pouch)
- Some fibres to levator ani portions.
- Superficial perineal branches (sensory):
- Become posterior scrotal nerves (in males) or posterior labial nerves (in females).
- Supply skin of:
- Posterior scrotum / labia majora
- Adjacent perineal skin.
3️⃣ Dorsal nerve of penis / clitoris
- Terminal branch of pudendal.
- Course:
- Runs anteriorly in deep perineal pouch, then
- Passes beneath the pubic symphysis, along dorsum of penis/clitoris with dorsal vessels.
- Supply:
- Major sensory nerve to glans penis / glans clitoris and dorsal penile/clitoral skin.
- Important for sexual sensation.
5. Structures Supplied (Summary)
Motor (somatic)
- External anal sphincter
- External urethral sphincter (through perineal branches)
- Perineal muscles:
- Superficial & deep transverse perineal
- Bulbospongiosus
- Ischiocavernosus
- Some fibres to levator ani (partly via branches around pelvic floor)
Sensory
- Anal region:
- Perianal skin & lower anal canal (below pectinate line) – via inferior rectal nerve.
- Perineum:
- Posterior perineal skin via posterior scrotal/labial nerves.
- External genitalia:
- Scrotum / labia majora (posterior aspect).
- Penis / clitoris, especially glans – via dorsal nerve of penis/clitoris.
6. Function (Clinical Logic)
- Somatic motor control of:
- Voluntary continence:
- External anal sphincter → fecal continence.
- External urethral sphincter → urinary continence.
- Stabilizing pelvic floor during straining, cough, etc.
- Somatic sensory:
- Perineal pain, touch, temperature.
- Sexual sensation in external genitalia.
7. Clinical Anatomy & Exam Points
1️⃣ Pudendal nerve block
- Used in obstetrics (perineal repair, instrumental delivery).
- Landmark:
- Ischial spine via vaginal route.
- Needle placed towards sacrospinous ligament, near pudendal as it hooks around the spine.
- Aim:
- Anaesthetize perineum & lower vagina (but not uterus or upper vagina – that’s visceral).
2️⃣ Injury / entrapment
- Causes:
- Childbirth trauma
- Pelvic surgery
- Prolonged cycling (compression in pudendal canal → “cyclist’s perineal syndrome”)
- Fractures of pelvic ring.
- Symptoms:
- Perineal pain or burning (pudendal neuralgia).
- Numbness in perineum/external genitalia.
- Weakness of external sphincters → fecal or urinary incontinence.
- Sexual dysfunction: erectile dysfunction / altered genital sensation.
3️⃣ Reflexes
- Anal wink reflex:
- Light perianal stimulation → contraction of external anal sphincter.
- Afferent & efferent mainly via pudendal (S2–S4).
- Bulbocavernosus reflex:
- Squeezing glans penis/clitoris → contraction of bulbospongiosus.
- Also tests S2–S4 pudendal integrity.
8. Key Differentiation (Exam Traps)
- Pudendal nerve vs pelvic splanchnic nerves:
- Pudendal: somatic, S2–S4, perineum & external genitalia, sphincters (voluntary).
- Pelvic splanchnic: parasympathetic, S2–S4, supply pelvic organs (bladder, rectum, genital organs viscerally).
- Pudendal vs ilioinguinal/genitofemoral cutaneous supply:
- Pudendal → perineum, posterior scrotum/labia, anus, genital shaft/glans.
- Ilioinguinal (L1) → root of penis/upper scrotum or mons pubis/labia majora (more anterior-superior).
- Genitofemoral → scrotum/labia (anterior), upper thigh patch.
If you’d like, next I can make 5 SBA + 10 T/F just on pudendal nerve (no answers first) to test whether this is fully in.
3. PELVIC SPLANCHNIC NERVES — “ONLY PARASYMPATHETIC IN BODY BELOW DIAPHRAGM”
Roots: S2–S4
This is the sacral parasympathetic outflow.
Functions:
- Motor to bladder → detrusor contraction
- Motor to rectum, sigmoid colon → peristalsis
- Erection (penile + clitoral) via vasodilation
- Afferent pain → bladder, cervix, rectum
Key clinical:
- Pelvic surgery can damage → constipation, urinary dysfunction
- Referred pain to posterior thigh (via posterior femoral cutaneous)
4. SUPERIOR GLUTEAL NERVE — "HIP STABILIZER"
Roots: L4–S1
Motor:
- Gluteus medius
- Gluteus minimus
- Tensor fascia lata
Clinical:
- Weakness → Trendelenburg gait
- Injury from injections in wrong quadrant (avoid upper medial!)
5. INFERIOR GLUTEAL NERVE — “POWER EXTENSION”
Roots: L5–S2
Motor:
- Gluteus maximus
Clinical:
- Difficulty rising from sitting / climbing stairs
- Loss of hip extension power
6. POSTERIOR FEMORAL CUTANEOUS NERVE — “LONG SENSORY STRIP”
Roots: S1–S3
Sensory:
- Buttock skin
- Posterior thigh
- Popliteal fossa
- Upper calf
Clinical:
- Pain/numbness along posterior thigh
- Misinterpreted as sciatica
⭐ OTHER NERVES — KNOW ONLY FUNCTIONS (VERY SHORT)
Nerve to obturator internus (L5–S2)
- Supplies obturator internus + superior gemellus
Nerve to quadratus femoris (L4–S1)
- Supplies quadratus femoris, inferior gemellus
- Also hip joint
Muscular S3–S4 branches
- Pelvic surface of levator ani + coccygeus
Perineal branch of S4
- Inferior pelvic diaphragm
- Skin of ischioanal fossa
⭐ SUPER SUMMARY TABLE (ALL YOU NEED)
Nerve | Roots | Motor | Sensory | Key Clinical |
Sciatic | L4–S3 | Hamstrings, leg, foot | Leg & foot | Sciatica, foot drop |
Pudendal | S2–S4 | Sphincters + perineal muscles | Perineum + genitalia | Pudendal block |
Pelvic splanchnic | S2–S4 | Bladder, rectum | Pelvic viscera | Erection, detrusor |
Sup. gluteal | L4–S1 | Glut med/min, TFL | — | Trendelenburg |
Inf. gluteal | L5–S2 | Glut maximus | — | Difficulty climbing |
Post. fem. cutaneous | S1–S3 | — | Buttock, post thigh | Sensory strip pain |
🎯 EXAM KEY UNDERSTANDINGS
If you remember ONLY these, you get 80%:
- Sciatic = biggest nerve → hamstrings + whole leg/foot.
- Pudendal = sphincters + perineum; S2–S4.
- Pelvic splanchnic = ONLY parasympathetic in lower abdomen → bladder/rectum + erection.
- Superior gluteal → hip abductors → Trendelenburg.
- Inferior gluteal → gluteus maximus → hip extension.
- Posterior femoral cutaneous → sensory strip of posterior thigh.