Owner
U
UntitledVerification
Tags


🟩 TABLE 1. Position, Extent & Relations of the Breast
Aspect | Details |
Anatomical plane | Lies in subcutaneous tissue (superficial fascia) of anterior thoracic wall |
Medial extent | Sternal edge |
Lateral extent | Near mid-axillary line |
Vertical extent | 2nd → 6th ribs |
Main muscle overlain | Pectoralis major |
Additional relations | Serratus anterior, small part over rectus sheath & external oblique |
Axillary extension | Axillary tail from upper outer quadrant |
Axillary tail position | Usually in subcutaneous fat |
Rare variation | May pierce deep fascia of axillary floor and lie close to axillary lymph nodes (oncologic importance) |
🟩 TABLE 2. Nipple, Areola & Duct System
Structure | Details |
Lactiferous ducts | 15–20 ducts, each draining one lobe |
Duct arrangement | Converge radially |
Duct openings | Open separately on the tip of nipple |
Lactiferous sinus | Dilated terminal part of each duct within nipple |
Nipple position | Projection just below centre of breast |
Nipple tissue | Contains smooth muscle fibres |
Nipple function | Smooth muscle contraction → nipple erection |
Areola | Pigmented skin surrounding nipple |
Areolar contents | Sebaceous glands, sweat glands, areolar glands |
Tubercles of Montgomery | Enlarged areolar glands |
Pregnancy change | Montgomery tubercles become prominent |
🟩 TABLE 3. Fascial Support, Shape & Mobility
Feature | Details |
Posterior capsule | Condensation of superficial fascia behind breast |
Fascial continuity | Upward continuation of Scarpa’s fascia |
Cooper’s ligaments | Fibrous bands from dermis → ducts → posterior capsule Crosses retro mammary space |
Function | Maintain shape & projection of young breast |
Ageing change | Atrophy → breast becomes pendulous |
Carcinoma effect | Fibrosis shortens ligaments → skin dimpling |
Lymphatic obstruction | Tethering + edema → peau d’orange |
Retromammary space | Loose connective tissue plane |
Retromammary relations | Between posterior capsule & pectoralis major fascia |
Functional role | Allows mobility of breast over chest wall |
🟩 TABLE 4. Male Breast (Comparison Table)
Feature | Male Breast |
Development | Rudimentary |
Lobules & alveoli | Absent |
Nipple & areola | Small |
Typical level | 4th intercostal space |
🟩 TABLE 5. Arterial Supply of the Breast
Artery | Contribution |
Lateral thoracic artery | Main contributor; branches curl around pectoralis major; some pierce muscle |
Internal thoracic artery | Perforating branches beside sternum |
Dominant perforators | 2nd & 3rd intercostal spaces |
Posterior intercostal arteries | Small perforating branches |
Thoracoacromial artery (pectoral branch) | Supplies upper breast |
Vascular pattern | Dense anastomosing network |
🟩 TABLE 6. Venous Drainage & Metastatic Routes
Aspect | Details |
Venous origin | Circumareolar venous plexus + glandular tissue |
Main drainage | Deep veins accompanying arteries |
Primary veins | Axillary vein, internal thoracic vein |
Additional drainage | Posterior intercostal veins |
Special connection | Posterior intercostal veins → internal vertebral venous plexus |
Clinical importance | Route for osseous metastasis |
🟩 TABLE 7. Lymphatic Drainage of the Breast (Complete)
Pathway | Details |
Subareolar plexus | Communicates with intramammary lymphatics |
Primary drainage (~75%) | Axillary lymph nodes |
Axillary node groups | Mainly anterior (pectoral); some posterior |
Direct axillary drainage | May go directly to central or apical nodes |
Medial breast drainage | Parasternal nodes along internal thoracic artery |
Intercostal pathway | Along intercostal arteries → posterior intercostal nodes |
Deltopectoral route | Infraclavicular nodes |
Interpectoral nodes | Between pectoralis major & minor |
Superficial connections | Opposite breast + anterior abdominal wall |
Inferior pathway | Abdominal extraperitoneal → diaphragm → posterior mediastinal nodes |
Direct supraclavicular route | To inferior deep cervical (supraclavicular) nodes |
Malignancy note | Minor routes enlarge when major channels blocked |
🟩 TABLE 8. Developmental Anatomy (Embryology)
Feature | Details |
Gland type | Modified sweat gland |
Time of origin | 4th week of gestation |
Embryonic structure | Mammary ridge (milk line) |
Germ layer | Ectoderm |
Milk line extent | Axilla → inguinal region |
Developmental anomalies | Supernumerary nipples/glands anywhere along milk line |
🟩 TABLE 9. Histological Organization & Life-Stage Changes
Stage | Structural Features |
Pre-puberty | No lobules |
Post-puberty (female) | Lobule formation begins |
Lobe structure | Lactiferous duct + tree-like ductal-lobular system |
Connective tissue | Lobes enclosed & supported |
Resting breast | Mostly fat + fibrous tissue, sparse glands |
Size variation | Depends on fat, not glandular tissue |
Pregnancy | Alveolar budding, marked enlargement |
Post-lactation | Involution of secretory tissue |
Post-menopause | Progressive atrophy of ducts & lobes |
🧠 FINAL EXAM LOCK (compressed)
Key Concept | One-Line Recall |
Core identity | Breast = superficial fascia organ |
Surface extent | 2nd–6th ribs, sternum → mid-axillary line |
Support | Cooper’s ligaments |
Main blood supply | Lateral thoracic artery |
Main lymph drainage | Axillary nodes (~75%) |
Development | Modified sweat gland from milk line |

Tanner Stages — ALL in ONE TABLE (exam-safe)
Stage | Female – Breast (B) | Female – Pubic Hair (PH) | Male – Genital (G) | Male – Pubic Hair (PH) |
1 | Prepubertal, nipple only | None | Prepubertal | None |
2 | Breast bud; areola enlarges | Sparse, lightly pigmented along labia | Testes enlarge, scrotum thins | Sparse hair at base of penis |
3 | Breast enlarges, no contour separation | Darker, coarser, curlier hair spreading | Penis lengthens | Darker, curlier hair |
4 | Secondary mound (areola + nipple) | Adult-type hair, not on thighs | Penis widens, glans develops; scrotum darkens | Adult-type hair, limited area |
5 | Adult breast; areola recesses | Adult distribution incl. medial thighs | Adult genitalia | Adult distribution incl. medial thighs |
Ultra-high-yield locks
- Girls: first sign = B2 (thelarche)
- Boys: first sign = G2 (testicular enlargement)
- Pubic hair ≠ gonadal maturity (androgen/adrenarche driven)
Breast — Logic-Based Anatomy & Development Note
1. Position, Extent & Surface Anatomy (Where it lies and what it overlies)
- The adult female breast (mammary gland) lies in the subcutaneous tissue (superficial fascia) of the anterior thoracic wall.
- Base extent (fairly constant despite size variation):
- Medial → lateral: from the sternal edge to near the mid-axillary line.
- Vertical: from the 2nd to the 6th ribs.
- Underlying structures:
- Mainly overlies pectoralis major.
- Also overlaps onto serratus anterior.
- A small part overlies the rectus sheath and external oblique muscle.
- Axillary extension:
- The upper outer quadrant may extend towards the axilla as the axillary tail.
- Usually lies in subcutaneous fat.
- Rarely, it may pierce the deep fascia of the axillary floor and lie close to axillary lymph nodes (important surgically and oncologically).
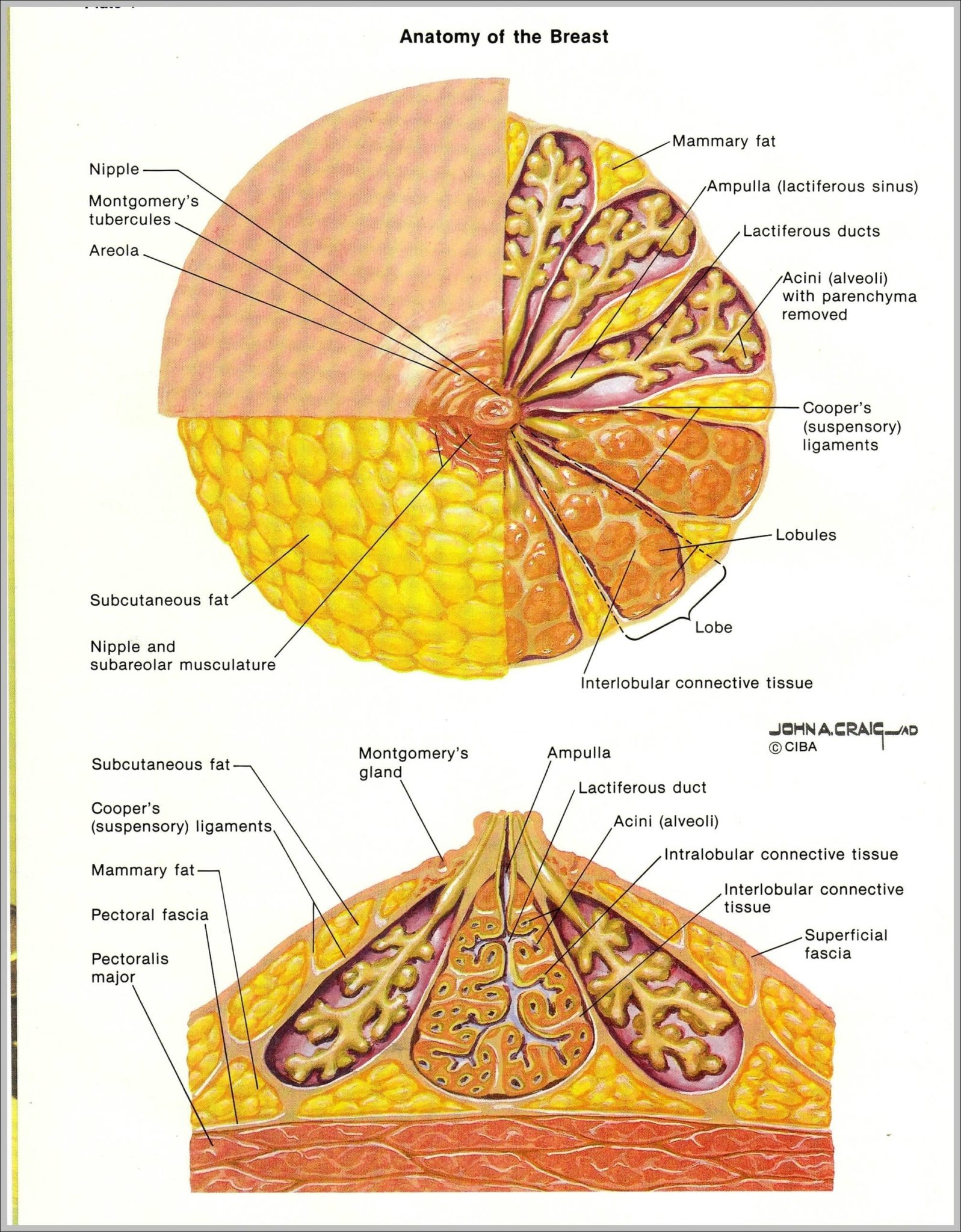
2. Nipple, Areola & Duct System (Functional surface structures)
- The breast is drained by 15–20 lactiferous ducts, each draining one lobe.
- These ducts:
- Converge radially.
- Open separately on the tip of the nipple.
- Nipple:
- A projection just below the centre of the breast.
- Contains smooth muscle fibres → contraction causes nipple erection.
- Areola:
- Pigmented skin surrounding the nipple.
- Contains:
- Large sebaceous glands
- Sweat glands
- Specialized areolar glands
- Lactiferous sinus:
- Each duct has a dilated terminal portion within the nipple.
- Tubercles of Montgomery:
- Small elevations on the areola.
- Represent enlarged areolar glands, especially prominent during pregnancy.
3. Fascial Support, Shape & Clinical Correlates
- Posterior capsule:
- Formed by condensation of superficial fascia behind the breast.
- This fascia is the upward continuation of Scarpa’s fascia from the abdomen.
- Suspensory ligaments of Cooper:
- Fibrous strands connecting:
- Dermis of the skin
- To breast ducts
- And to the posterior capsule
- Functions and clinical effects:
- Maintain the shape and projection of the young breast.
- With age-related atrophy → breast becomes pendulous.
- In carcinoma, fibrosis shortens these ligaments → skin dimpling.
- In malignant lymphatic obstruction, tethering + edema → peau d’orange appearance.
- Retromammary space:
- A layer of loose connective tissue.
- Lies between:
- Posterior capsule of breast
- Fascia over pectoralis major
- Allows mobility of the breast over the chest wall.
4. Male Breast (Comparison point)
- Resembles a rudimentary female breast.
- No lobules or alveoli.
- Small nipple and areola usually lie over the 4th intercostal space.
5. Blood Supply (Arteries → Veins → Metastatic relevance)
Arterial supply (rich anastomotic network)
- Lateral thoracic artery (main contributor):
- Branches curl around the border of pectoralis major.
- Other branches pierce the muscle.
- Internal thoracic artery:
- Sends perforating branches through intercostal spaces beside the sternum.
- 2nd and 3rd intercostal spaces supply the largest branches.
- Posterior intercostal arteries:
- Small perforating branches.
- Thoracoacromial artery (pectoral branch):
- Supplies the upper part of the breast.
- All arteries form a dense anastomosing network.
Venous drainage
- From:
- Circumareolar venous plexus
- Glandular tissue
- Drains mainly via deep veins accompanying arteries to:
- Axillary vein
- Internal thoracic vein
- Some blood drains to posterior intercostal veins →
- Connects to internal vertebral venous plexus
- Provides a route for metastatic spread to bone.
6. Lymphatic Drainage (Major and minor pathways)
- Subareolar lymphatic plexus:
- Communicates with lymphatics within the breast.
- Primary drainage (~75%):
- To axillary lymph nodes:
- Mainly anterior (pectoral) nodes
- Some to posterior nodes
- Direct drainage to central or apical nodes can occur.
- Medial breast drainage:
- To parasternal nodes along the internal thoracic artery.
- Additional pathways:
- Along intercostal arteries → posterior intercostal nodes.
- Occasionally to:
- Infraclavicular nodes in the deltopectoral groove
- Interpectoral nodes (between pectoralis major and minor).
- Superficial lymphatic connections:
- With the opposite breast.
- With the anterior abdominal wall.
- From abdominal extraperitoneal tissues → through diaphragm → posterior mediastinal nodes.
- Direct supraclavicular drainage:
- Possible to inferior deep cervical (supraclavicular) nodes.
- Clinical note:
- Minor pathways usually become significant only when major channels are blocked by malignancy.
7. Development & Histological Organization
Embryological origin
- The breast is a modified sweat gland.
- Develops as early as the 4th week of gestation.
- Originates from a thickened mammary ridge (milk line) of ectoderm:
- Extends from axilla to inguinal region.
- Supernumerary nipples or glands may appear anywhere along this line.
Post-pubertal and adult structure
- Lobule formation occurs only in females and after puberty.
- Each lactiferous duct connects to a tree-like branching system of:
- Ducts
- Lobules
- These structures are:
- Intermingled
- Enclosed by connective tissue
- Together form a lobe of the gland.
Functional states across life
- Resting (non-lactating) breast:
- Composed mainly of fat and fibrous tissue.
- Size variation depends on fat content, not glandular tissue.
- Glandular tissue is sparse.
- Pregnancy:
- Alveoli bud from smaller ducts.
- Breast enlarges significantly in preparation for lactation.
- Post-lactation:
- Involution of secretory tissue.
- After menopause:
- Progressive atrophy of lobes and ducts.
One-line logic lock (exam-safe)
Breast = superficial fascia organ (2nd–6th ribs, sternum → mid-axillary line), supported by Cooper’s ligaments, drained mainly to axillary nodes, supplied chiefly by lateral thoracic artery, and developmentally a modified sweat gland arising from the milk line.