STRUCTURE
What the hypothalamus is
- The hypothalamus is the portion of the anterior end of the diencephalon.
- It lies:
- Below the hypothalamic sulcus
- In front of the interpeduncular nuclei
- It is composed of multiple nuclei and nuclear areas, each specialized for regulatory roles.
Core logic:
Location below the thalamus + proximity to brainstem + multiple nuclei = ideal position for integrating neural, endocrine, and autonomic control.
2. AFFERENT & EFFERENT CONNECTIONS OF THE HYPOTHALAMUS
General properties of hypothalamic pathways
- Principal afferent and efferent pathways are mostly unmyelinated.
- Many connections link the hypothalamus to the limbic system.
- Additional major connections exist with:
- Midbrain tegmentum
- Pons
- Hindbrain
Logic:
Unmyelinated fibers → slower but sustained signaling → ideal for homeostatic regulation, not rapid motor control.
Monoaminergic & Peptidergic Inputs and Outputs
Norepinephrine pathways
- Norepinephrine-secreting neurons
- Cell bodies located in the hindbrain
- Axons terminate in many different parts of the hypothalamus
Dopamine (intrahypothalamic system)
- Dopamine-secreting neurons
- Cell bodies in the arcuate nucleus
- Axons terminate on or near capillaries in the median eminence
- These capillaries form the portal vessels
Logic:
Dopamine → median eminence → portal blood → direct control of anterior pituitary secretion
Serotonin pathways
- Serotonin-secreting neurons
- Originate from the raphe nuclei
- Project to the hypothalamus
Epinephrine pathways
- Epinephrine-secreting neurons
- Cell bodies in the hindbrain
- Axons terminate in the ventral hypothalamus
Oxytocin & vasopressin projections
- Neurons located in the paraventricular nucleus
- Secrete oxytocin and vasopressin
- Project to:
- Hindbrain
- Spinal cord
Logic:
These projections allow hypothalamic hormones to influence autonomic and behavioral responses, not just pituitary output.
3. RELATIONSHIP TO THE PITUITARY GLAND
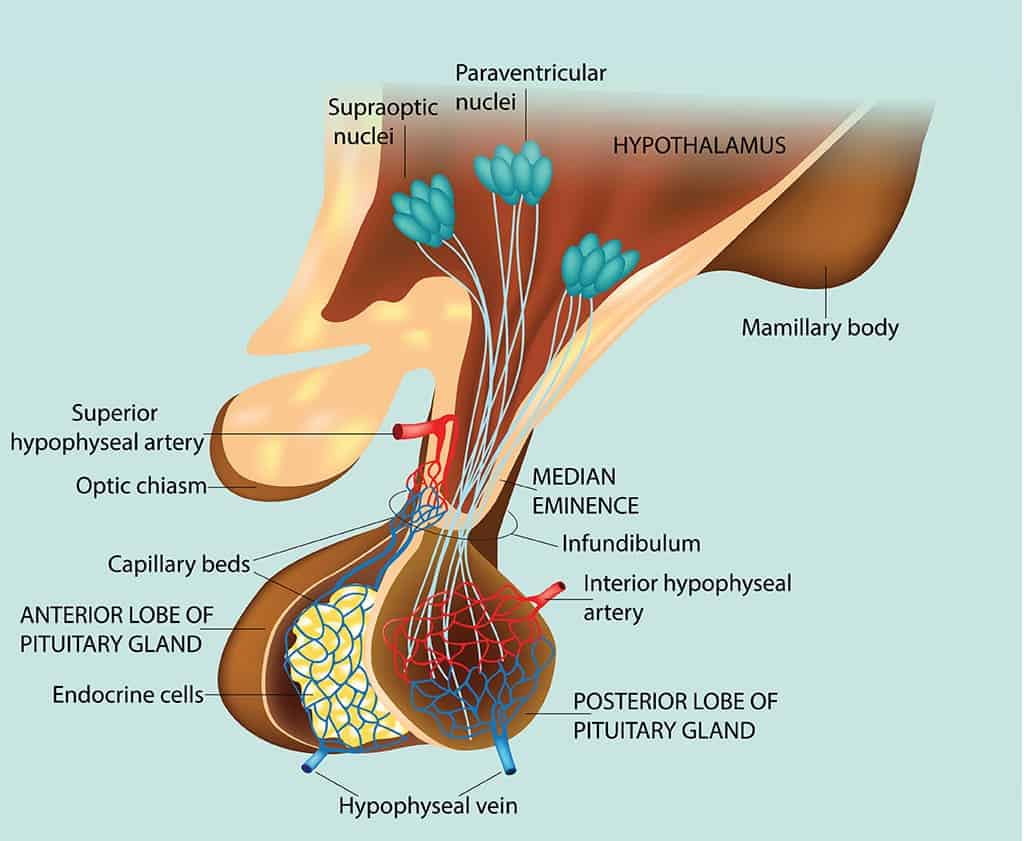
Posterior pituitary (Neurohypophysis)
Embryology
- Arises as an evagination of the floor of the third ventricle
Structural composition
- Composed largely of axon endings
- Axons arise from cell bodies in:
- Supraoptic nucleus
- Paraventricular nucleus
Pathway
- Axons pass via the hypothalamohypophysial tract
- Terminate in the posterior pituitary
Fiber distribution
- Most supraoptic fibers → end in posterior pituitary
- Some paraventricular fibers → end in the median eminence
Anterior pituitary (Adenohypophysis)
Embryology
- Arises from Rathke pouch
- Rathke pouch = evagination from the roof of the pharynx
Neural connections
- Sympathetic fibers reach the anterior pituitary via its capsule
- Parasympathetic fibers reach it via the petrosal nerves
- Few or no nerve fibers pass directly from hypothalamus to anterior pituitary
4. PORTAL HYPOPHYSIAL SYSTEM (CRITICAL LOGIC)
Primary capillary plexus
- Formed by arterial twigs from:
- Carotid arteries
- Circle of Willis
- These twigs create fenestrated capillaries
- Located on the ventral surface of the hypothalamus
Median eminence
- Capillary loops penetrate the median eminence
- Defined as the portion of ventral hypothalamus from which portal vessels arise
- Lies outside the blood–brain barrier
Portal vessels
- Capillaries drain into sinusoidal portal hypophysial vessels
- These vessels carry blood:
- Down the pituitary stalk
- To capillaries of the anterior pituitary
Key property
- System begins and ends in capillaries
- Does not pass through the heart
- Therefore, it is a true portal system
Arterial supply fact (exam favorite)
- In birds and some mammals, including humans:
- There is no other arterial supply to the anterior pituitary
- Except:
- Capsular vessels
- Anastomotic connections from posterior pituitary capillaries
5. FUNCTIONAL PRINCIPLE OF THE HYPOTHALAMUS
Core concept
- All hypothalamic functions involve:
- A specific stimulus
- Producing a specific response
Types of functions
- Some are visceral reflexes
- Others involve complex behavioral and emotional responses
- All are integrated regulatory mechanisms
6. PRINCIPAL HYPOTHALAMIC FUNCTIONS (TABLE 17–1 — FULL LOGIC)
A. TEMPERATURE REGULATION
Afferents from
- Temperature receptors in:
- Skin
- Deep tissues
- Spinal cord
- Hypothalamus
- Other brain regions
Integrating areas
- Anterior hypothalamus → response to heat
- Posterior hypothalamus → response to cold
B. NEUROENDOCRINE CONTROL
Catecholamines
- Afferents: Limbic areas concerned with emotion
- Integrating areas: Dorsal and posterior hypothalamus
Vasopressin
- Afferents:
- Osmoreceptors
- “Volume receptors”
- Others
- Integrating areas:
- Supraoptic nucleus
- Paraventricular nucleus
Oxytocin
- Afferents:
- Touch receptors in breast
- Uterus
- Genitalia
- Integrating areas:
- Supraoptic nucleus
- Paraventricular nucleus
Thyroid-stimulating hormone (via TRH)
- Afferents:
- Temperature receptors in infants (perhaps others)
- Integrating areas:
- Paraventricular nucleus and neighboring areas
ACTH & β-LPH (via CRH)
- Afferents:
- Limbic system (emotional stimuli)
- Reticular formation (“systemic” stimuli)
- Hypothalamic & anterior pituitary cells sensitive to blood cortisol
- Suprachiasmatic nuclei (diurnal rhythm)
- Integrating areas:
- Paraventricular nucleus
FSH & LH (via GnRH)
- Afferents:
- Hypothalamic cells sensitive to estrogens
- Eyes
- Touch receptors in skin and genitalia (reflex ovulating species)
- Integrating areas:
- Preoptic area
- Other hypothalamic areas
Prolactin (via PIH & PRH)
- Afferents:
- Touch receptors in breasts
- Other unknown receptors
- Integrating areas:
- Arcuate nucleus
- Other hypothalamic areas
- (Hypothalamus inhibits secretion)
Growth hormone
- Afferents:
- Unknown receptors
- Integrating areas:
- Periventricular nucleus
- Arcuate nucleus
C. APPETITIVE BEHAVIOR
Thirst
- Afferents:
- Osmoreceptors (likely in organum vasculosum of lamina terminalis)
- Angiotensin II uptake in subfornical organ
- Integrating area:
- Lateral superior hypothalamus
Hunger
- Afferents:
- Glucostat cells (rate of glucose utilization)
- Leptin receptors
- Other polypeptide receptors
- Integrating areas:
- Ventromedial nucleus
- Arcuate nucleus
- Paraventricular nucleus
- Lateral hypothalamus
Sexual behavior
- Afferents:
- Cells sensitive to circulating estrogen, androgen, others
- Integrating areas:
- Anterior ventral hypothalamus
- Piriform cortex (male)
D. DEFENSIVE REACTIONS (FEAR, RAGE)
- Afferents:
- Sense organs
- Neocortex (paths unknown)
- Integrating areas:
- Diffuse limbic system
- Hypothalamus
E. CONTROL OF BODY RHYTHMS
- Afferents:
- Retina via retinohypothalamic fibers
- Integrating area:
- Suprachiasmatic nucleus
FINAL CORE LOGIC LOCK (EXAM SENTENCE)
The hypothalamus is a ventral diencephalic structure composed of multiple nuclei that integrate limbic, autonomic, endocrine, and sensory inputs to produce stimulus-specific homeostatic, behavioral, and neuroendocrine responses via direct neural connections and a unique portal vascular system.
CONTROL OF POSTERIOR PITUITARY SECRETION
Vasopressin (ADH) & Oxytocin
1️⃣ Posterior Pituitary Hormones – Core Identity
- The posterior pituitary secretes two hormones:
- Arginine vasopressin (AVP)
- Oxytocin
- Species variation:
- In hippopotami and most pigs, arginine is replaced by lysine → lysine vasopressin.
- Some pigs and marsupials contain a mixture of arginine and lysine vasopressin.
- Structural property:
- Both hormones are nonapeptides (nanonpeptides).
- They contain a disulfide ring at one end → important for structure and function.
2️⃣ Site of Synthesis & Neuronal Nature (Big Picture Logic)
- Posterior pituitary hormones are not synthesized in the posterior pituitary itself.
- They are synthesized in magnocellular neurons located in:
- Supraoptic nucleus
- Paraventricular nucleus
- These neurons:
- Produce hormone in their cell bodies
- Transport hormone down their axons
- Release hormone from nerve endings in the posterior pituitary
- Therefore:
- Oxytocin and vasopressin are neural hormones
- Hormones secreted into blood by neurons
- Term neurosecretion:
- Originally used to describe hormone secretion by neurons
- Somewhat misleading because all neurons secrete chemical messengers
3️⃣ Neuronal Segregation (Important Clarification)
- Some magnocellular neurons synthesize oxytocin
- Others synthesize vasopressin
- Both nuclei (supraoptic + paraventricular) contain:
- Oxytocin-secreting neurons
- Vasopressin-secreting neurons
4️⃣ Hormone Biosynthesis – Precursor Logic (Very High Yield)
A. General Peptide Hormone Principle
- Like all peptide hormones:
- Synthesized as larger precursor molecules
- Undergo post-translational processing
B. Vasopressin Precursor
- Precursor molecule: Prepropressophysin
- Composition (in order):
- 19-amino-acid leader (signal) sequence
- Vasopressin
- Neurophysin II
- Glycopeptide
C. Oxytocin Precursor
- Precursor molecule: Prepro-oxyphysin
- Composition:
- Leader sequence
- Oxytocin
- Neurophysin I
- No glycopeptide (key difference from vasopressin precursor)
D. Role of Neurophysins
- Neurophysin I → associated with oxytocin
- Neurophysin II → associated with vasopressin
- Initially thought to be binding proteins
- Now known to be integral parts of precursor molecules
- Function remains unknown
5️⃣ Intracellular Processing & Axonal Transport
- Precursor synthesis:
- Occurs on ribosomes in neuron cell bodies
- Processing steps:
- Leader sequence removed in endoplasmic reticulum
- Molecules packaged into secretory granules in Golgi
- Granules transported down axons by axoplasmic flow
- Storage:
- Granules accumulate in axon terminals as Herring bodies
- Easily visualized histologically
- During transport:
- Precursor cleavage occurs
- Final granule contents:
- Free vasopressin or oxytocin
- Corresponding neurophysin
- Glycopeptide (only with vasopressin)
- All components are secreted, but functions other than hormones are unknown
6️⃣ Electrical Activity & Hormone Release Mechanism
- Magnocellular neurons:
- Generate and conduct action potentials
- Hormone release mechanism:
- Action potentials reach nerve endings
- Trigger Ca²⁺-dependent exocytosis
- Basal firing (anesthetized rats):
- Silent or low irregular firing (0.1–3 spikes/sec)
7️⃣ Differential Firing Patterns (Key Functional Logic)
A. Oxytocin Neurons
- Stimulus: Nipple stimulation
- Response:
- Synchronous
- High-frequency discharge
- Occurs after appreciable latency
- Effect:
- Pulsatile oxytocin release
- Milk ejection
B. Vasopressin Neurons
- Stimuli:
- ↑ Plasma osmolality (dehydration)
- ↓ Blood volume (hemorrhage)
- Response pattern:
- Initial steady increase in firing
- Followed by phasic bursting
- Alternating high-frequency bursts
- Periods of electrical silence
- Bursts:
- Not synchronous across neurons
- Functional advantage:
- Maintains prolonged vasopressin secretion
- Contrast:
- Oxytocin → short, synchronous bursts
- Vasopressin → sustained, phasic output
8️⃣ Vasopressin & Oxytocin Outside Posterior Pituitary
- Vasopressin-secreting neurons:
- Present in suprachiasmatic nuclei
- Paraventricular projections:
- To brainstem and spinal cord
- Involved in cardiovascular control
- Peripheral synthesis:
- Vasopressin & oxytocin → gonads
- Vasopressin & oxytocin → adrenal cortex
- Oxytocin → thymus
- Functions in these locations: not established
9️⃣ Vasopressin Receptors (Exam-Critical)
- Three receptor types:
- V1A
- V1B
- V2
- All are G-protein–coupled receptors
- Signaling pathways:
- V1A & V1B → phosphatidylinositol hydrolysis → ↑ intracellular Ca²⁺
- V2 → Gs → ↑ cAMP
🔟 Physiologic Effects of Vasopressin (ADH)
- Primary role: Water retention
- Kidney action:
- ↑ Permeability of collecting ducts
- Water moves into hypertonic renal medullary interstitium
- Consequences:
- Urine becomes concentrated
- Urine volume decreases
- Net effect: water retained in excess of solute
- → ↓ Effective osmotic pressure of body fluids
- Absence of vasopressin:
- Urine hypotonic to plasma
- ↑ Urine volume
- Net water loss
- ↑ Body fluid osmolality
1️⃣1️⃣ Oxytocin Receptors & Cellular Action
- Acts mainly on:
- Uterus
- Breasts
- Also implicated in:
- Luteolysis
- Receptor:
- G-protein–coupled oxytocin receptor
- Present in:
- Myometrium
- Mammary tissue
- Ovary
- Mechanism:
- ↑ Intracellular Ca²⁺
1️⃣2️⃣ Milk Ejection Reflex (Classic Neuroendocrine Reflex)
Mechanism Chain
- Oxytocin contracts myoepithelial cells
- Milk squeezed from alveoli
- Milk enters large ducts (sinuses)
- Milk exits via nipple
Reflex Control
- Receptors: Touch receptors in breast (especially nipple)
- Afferent pathway:
- Somatic sensory pathways
- → Supraoptic & paraventricular nuclei
- Efferent:
- Oxytocin secretion from posterior pituitary
- Trigger:
- Infant suckling
- Additional stimuli:
- Genital stimulation
- Emotional stimuli
- Can cause spontaneous milk ejection
1️⃣3️⃣ Oxytocin & Uterine Function
- Causes uterine smooth muscle contraction
- Hormonal modulation:
- Estrogen → increases sensitivity
- Progesterone → inhibits sensitivity
- Progesterone mechanism:
- Direct action on oxytocin receptors
- Late pregnancy:
- ↑ Oxytocin receptor number
- ↑ Oxytocin receptor mRNA
- Labor:
- Plasma oxytocin initially normal
- ↑ receptor density → contractions begin
- Cervical dilation + fetal descent:
- Afferent impulses to hypothalamic nuclei
- ↑ Oxytocin secretion
- Positive feedback:
- Oxytocin → contractions → more oxytocin
- Local production:
- Oxytocin concentration increased in uterus
- Locally produced oxytocin may contribute
1️⃣4️⃣ Additional Actions of Oxytocin
- Non-pregnant uterus:
- May facilitate sperm transport
- Coitus:
- Genital stimulation → oxytocin release
- Role in sperm transport not proven
- Stress:
- ↑ Oxytocin secretion
- Alcohol:
- Inhibits oxytocin secretion (similar to vasopressin)
- Males:
- Circulating oxytocin ↑ at ejaculation
- May increase contraction of vas deferens
- Facilitates sperm propulsion
🧠 ONE-LINE MASTER LOGIC (Exam Compression)
Posterior pituitary hormones are synthesized as peptide precursors in magnocellular hypothalamic neurons, processed with neurophysins, transported to the posterior pituitary, and released by Ca²⁺-dependent exocytosis in distinct firing patterns—phasic for vasopressin (water balance) and synchronous for oxytocin (milk ejection and parturition).
Control of Anterior Pituitary Secretion — Logic-Based, Zero-Omission Note

1️⃣ Big Picture (Master Logic)
- The anterior pituitary does NOT act independently.
- Its secretion is chemically controlled by the hypothalamus.
- Control signals are hypophysiotropic hormones delivered via the portal hypophysial circulation, not by direct nerves.
- Therefore:
Hypothalamus → portal blood → anterior pituitary → peripheral endocrine glands
2️⃣ What the Anterior Pituitary Secretes (Complete List)
Six principal hormones
- ACTH (adrenocorticotropic hormone; corticotropin)
- TSH (thyroid-stimulating hormone; thyrotropin)
- Growth hormone (GH)
- FSH (follicle-stimulating hormone)
- LH (luteinizing hormone)
- Prolactin (PRL)
Additional peptide
- β-Lipotropin (β-LPH)
- Secreted with ACTH
- Physiologic role unknown
3️⃣ Unique Feature of Hypothalamic Control
- Hypothalamus:
- Stimulates secretion of:
- ACTH
- β-LPH
- TSH
- GH
- FSH
- LH
- Inhibits prolactin TONICALLY
- Prolactin is the only anterior pituitary hormone under dominant inhibitory control
👉 Key logic:
If the hypothalamus is damaged → prolactin increases, others usually fall.
4️⃣ Nature of Hypothalamic Control (How Signals Travel)
- Control is via chemical agents, not action potentials.
- These agents:
- Are secreted into portal hypophysial vessels
- Travel from median eminence → anterior pituitary
- Reach highest concentration in portal blood
- Only small amounts enter systemic circulation
Terminology update:
- Old terms: releasing factors / inhibiting factors
- Correct term: Hypophysiotropic hormones
- Appropriate because they are blood-borne hormones acting at a distance
5️⃣ Hypophysiotropic Hormones — Complete & Exact List
Six established hypothalamic hormones
Hypothalamic hormone | Also called | Primary pituitary effect |
CRH | Corticotropin-releasing hormone | ↑ ACTH + β-LPH |
TRH | Thyrotropin-releasing hormone | ↑ TSH, ↑ Prolactin |
GRH (GHRH) | Growth hormone–releasing hormone | ↑ GH |
GIH | Somatostatin | ↓ GH, ↓ TSH |
LHRH | GnRH | ↑ LH and ↑ FSH |
PIH | Dopamine | ↓ Prolactin |
6️⃣ Prolactin Regulation — Special Case
- No single proven physiologic PRH
- Substances that stimulate prolactin:
- TRH
- VIP
- Other hypothalamic peptides
- A 31-amino-acid hypothalamic polypeptide:
- Identified via an orphan receptor
- Stimulates prolactin secretion
- Physiologic role still unconfirmed
👉 Bottom line:
- Dopamine = dominant regulator
- Prolactin rises when dopamine inhibition is removed
7️⃣ Why There Is NO Separate FSH-Releasing Hormone
- GnRH stimulates BOTH LH and FSH
- Evidence suggests:
- A separate FSH-RH does not exist
8️⃣ Molecular Biology Facts (Often Forgotten)
- Gene structures & preprohormones are known for:
- TRH
- GnRH
- Somatostatin
- CRH
- GRH
Important detail:
- PreproTRH contains SIX copies of TRH
- Some preprohormones contain additional bioactive peptides
9️⃣ Where Hypophysiotropic Hormones Are Released
Median eminence of the hypothalamus
- Characteristics:
- Few neuronal cell bodies
- Many nerve terminals
- Close to capillary loops
- Portal vessels originate here
👉 Structural logic:
Neurons → median eminence → portal blood → anterior pituitary
🔟 Location of Hypothalamic Neuron Cell Bodies
Hormone | Neuronal origin |
GnRH | Medial preoptic area |
Somatostatin | Periventricular nuclei |
TRH | Medial paraventricular nuclei |
CRH | Medial paraventricular nuclei |
GRH | Arcuate nuclei |
Dopamine (PIH) | Arcuate nuclei |
Oxytocin & Vasopressin | Separate magnocellular neurons (shown for contrast) |
1️⃣1️⃣ One Hypothalamic Hormone → Multiple Pituitary Effects
Hormone | Additional actions |
GnRH | Stimulates FSH + LH |
TRH | Stimulates prolactin + TSH |
Somatostatin | Inhibits GH + TSH |
Somatostatin (pathologic) | Inhibits excess ACTH (Nelson syndrome) |
CRH | Stimulates ACTH + β-LPH |
1️⃣2️⃣ Actions Outside the Pituitary
Hypophysiotropic hormones also act as:
- Neurotransmitters in:
- Brain
- Retina
- Autonomic nervous system
Peripheral locations:
- Somatostatin → pancreatic islets
- GRH → secreted by pancreatic tumors
- Somatostatin & TRH → gastrointestinal tract
1️⃣3️⃣ Receptors & Signal Transduction
- Most hypophysiotropic hormone receptors are:
- G-protein–coupled receptors (GPCRs)
CRH receptors:
- hCRH-RI
- hCRH-RII
- Widely distributed in brain
- Physiologic role not fully defined
CRH-binding protein:
- Found in:
- Peripheral circulation → inactivates CRH
- Cytoplasm of corticotropes
- Possible role:
- Receptor internalization
- Exact function unknown
👉 Other hypophysiotropic hormones:
- No known binding proteins
1️⃣4️⃣ Why This Matters (Physiologic Significance)
- Hypothalamus integrates:
- Internal environment
- External environment
- Nervous system inputs →
- Motor responses
- Hormonal output adjustments
- This allows endocrine secretion to match physiologic demand
1️⃣5️⃣ Clinical Implications of Hypothalamic Disease
Manifestations include:
- Neurologic defects
- Endocrine abnormalities
- Metabolic disturbances
- Hyperphagia
- Hyperthermia
👉 Clinical rule:
- Always consider hypothalamic pathology in:
- Pituitary dysfunction
- Isolated deficiency of a single tropic hormone
1️⃣6️⃣ Kallmann Syndrome — Logic Explained
Core features:
- Hypogonadotropic hypogonadism
- Hyposmia or anosmia
Embryologic mechanism:
- GnRH neurons:
- Originate in nasal placode
- Migrate along olfactory nerves
- Enter hypothalamus
- Failure of migration →
- No GnRH in hypothalamus
- No pubertal gonadal maturation
Genetics:
- Common cause:
- KALIG1 gene mutation
- X-linked
- Codes for an adhesion molecule
- More common in men
- Also occurs in women via other genetic defects
🧠 Final Integrated Logic Line
Anterior pituitary hormone secretion is governed by hypothalamic hypophysiotropic hormones released at the median eminence into portal vessels, acting via GPCRs to finely tune endocrine output according to environmental and physiologic demands, with prolactin uniquely under tonic inhibitory control and clinical disorders arising when neuronal development, migration, or signaling fails.
TEMPERATURE REGULATION
1) Core Principle: Why temperature must be controlled
- Heat is produced by:
- Muscular exercise.
- Assimilation of food.
- All vital processes that contribute to basal metabolic rate (BMR).
- Heat is lost by:
- Radiation.
- Conduction.
- Vaporization of water in respiratory passages and on skin.
- Small amounts via urine and feces.
- Body temperature is determined by the balance:
- Heat production minus heat loss.
- Constant temperature matters because:
- Chemical reaction speed varies with temperature.
- Enzymes have narrow optimal temperature ranges.
- Normal body function depends on relatively constant temperature.
2) Animals: who can regulate and who cannot
- Invertebrates:
- Generally cannot adjust body temperature.
- Body temperature is at the mercy of environment.
- Vertebrates:
- Evolved mechanisms to maintain body temperature by adjusting heat production and heat loss.
- Poikilotherms (“cold-blooded”):
- Reptiles, amphibians, fish.
- Mechanisms are rudimentary.
- Body temperature fluctuates over a considerable range.
- Homeotherms (“warm-blooded”):
- Birds and mammals.
- Reflex responses integrated primarily in hypothalamus maintain temperature within a narrow range despite environmental fluctuations.
- Hibernating mammals (partial exception):
- Homeothermic while awake.
- During hibernation, body temperature falls.
3) Normal body temperature: human facts (with measurement logic)
- Traditional normal oral temperature: 37°C (98.6°F).
- Large series of normal young adults:
- Morning oral temperature mean: 36.7°C.
- Standard deviation: 0.2°C.
- 95% range (mean ± 1.96 SD): 36.3–37.1°C (97.3–98.8°F).
- Different body parts have different temperatures:
- Extremities are generally cooler.
- Scrotum is regulated at 32°C.
- Rectal temperature represents core temperature and varies least with environmental change.
- Oral temperature is normally 0.5°C lower than rectal temperature.
- Oral temperature is affected by:
- Hot or cold fluids.
- Gum chewing.
- Smoking.
- Mouth breathing.
- Circadian rhythm in core temperature:
- Regular fluctuation: 0.5–0.7°C.
- In night sleepers/day-wakers (even hospitalized at bed rest):
- Lowest at about 6:00 AM.
- Highest in evenings.
- Lowest during sleep.
- Slightly higher when awake but relaxed.
- Rises with activity.
- Monthly cycle in women:
- Rise in basal temperature at ovulation.
- Children:
- Temperature regulation less precise.
- May normally be about 0.5°C above established adult norm.
4) Temperature changes in common physiologic states
- Exercise:
- Heat from muscular contraction accumulates.
- Rectal temperature can rise as high as 40°C (104°F).
- Rise is due to:
- Heat-dissipating mechanisms being unable to handle the increased heat.
- Evidence also suggests a higher activation temperature for heat-dissipating mechanisms during exercise (a shifted activation threshold).
- Emotional excitement:
- Slight temperature rise.
- Likely due to unconscious muscle tensing.
- Thyroid state:
- High metabolic rate (hyperthyroidism): chronic elevation up to 0.5°C.
- Low metabolic rate (hypothyroidism): lowered temperature.
- Constitutional hyperthermia:
- Some apparently normal adults chronically have temperature above normal range.
5) Heat production: sources and hormonal control
- Heat is continuously produced by basic chemical reactions.
- Food ingestion increases heat production.
- Major source of heat: skeletal muscle contraction.
- Endocrine variation of heat production without food or exertion:
- Epinephrine and norepinephrine:
- Rapid but short-lived increase in heat production.
- Thyroid hormones:
- Slowly developing but prolonged increase.
- Sympathetic discharge changes with nutrition:
- Decreases during fasting.
- Increases by feeding.
- Brown fat (especially in infants):
- High metabolic rate.
- Thermogenic function likened to an electric blanket.
6) Heat loss mechanisms: physical processes + skin blood flow logic
A) Heat transfer when environmental temperature is below body temperature
- Conduction:
- Heat exchange between objects/substances in contact at different temperatures.
- Thermal energy transfer occurs due to molecular motion and collisions.
- Heat transferred is proportional to temperature difference (thermal gradient).
- Convection:
- Movement of molecules away from area of contact, aiding conduction.
- Example logic:
- Warm air rises, cool air falls, bringing new air into contact.
- Greatly increased by:
- Movement of the object in the medium (swimming).
- Movement of the medium past the object (fan blowing air).
- Radiation:
- Transfer via infrared electromagnetic radiation between objects not in contact.
- In cold environments:
- Heat lost by conduction to air and radiation to cool objects.
- In hot environments (above body temperature):
- Conduction and radiation transfer heat to the person, increasing heat load.
- Practical consequences:
- Feeling chilly in a room with cold walls even if air is warm (radiation).
- On cold but sunny days, reflected heat from bright objects (snow) warms appreciably.
B) Skin temperature and blood flow: tissue conductance
- Skin temperature strongly determines heat loss/gain because conduction occurs surface-to-surface.
- Heat reaching skin from deep tissues is controlled by skin blood flow:
- Cutaneous vasodilation:
- Warm blood wells into skin.
- Increases heat transfer to environment.
- Maximal vasoconstriction:
- Heat held centrally.
- Tissue conductance:
- The rate at which heat is transferred from deep tissues to the skin.
C) Insulation: fur/feathers/hair/clothing + horripilation logic
- Birds and mammals have feathers/hair/fur:
- Heat conducts from skin to trapped air layer, then to outside.
- Increasing trapped layer thickness reduces heat transfer and reduces heat loss (or heat gain in hot environments).
- Horripilation:
- Erection of hairs increases trapped air layer, reducing heat transfer.
- In humans, goose pimples are the visible manifestation of cold-induced contraction of piloerector muscles attached to the sparse hair supply.
- Clothing:
- Adds trapped air layers.
- Heat transfer steps:
- Skin to trapped air inside clothing.
- Inside clothing to outside clothing.
- Outside clothing to environment.
- How warm/cool clothing feels depends mainly on:
- Texture and thickness (heat transfer magnitude across clothing).
- Size of trapped warm-air layer.
- Color effect:
- Dark clothes absorb radiated heat.
- Light-colored clothes reflect it outward.
D) Vaporization: sweating + respiration + panting
- Vaporization of 1 g water removes about 0.6 kcal heat.
- Insensible water loss:
- Occurs all the time.
- About 50 mL/h in humans.
- Sweating:
- Increased sweat secretion increases potential heat loss.
- Effectiveness depends on environmental humidity.
- People feel hotter on humid days partly due to decreased sweat vaporization.
- Even when sweat vaporization is complete, humid environments feel warmer than dry environments:
- Reason unknown.
- Proposed link: sweat spreads over greater skin area before evaporating.
- Sweat secretion can reach 1600 mL/h during exertion in heat.
- In dry atmosphere, most of this sweat is vaporized.
- Heat loss via vaporization varies from 30 to over 900 kcal/h.
- Panting (some mammals):
- Rapid shallow breathing increases water vaporization in mouth/respiratory passages.
- Increases heat loss.
- Shallow breathing produces relatively little change in alveolar air composition.
- Relative contribution changes with environmental temperature:
- At 21°C in resting humans: vaporization is minor.
- As environmental temperature approaches body temperature:
- Radiation losses decline.
- Vaporization losses increase.
7) Thermoregulatory mechanisms: response sets and triggers
- Thermoregulatory responses include:
- Autonomic.
- Somatic.
- Endocrine.
- Behavioral.
- Two functional groups:
- Heat-loss / heat-production decrease group.
- Heat-loss decrease / heat-production increase group.
- General rule:
- Heat exposure stimulates heat-loss responses and inhibits heat-gain responses.
- Cold exposure stimulates heat-gain responses and inhibits heat-loss responses.
Table 17–4 content (complete)
Mechanisms activated by cold
- Shivering.
- Hunger.
- Increased voluntary activity.
- Increased secretion of norepinephrine and epinephrine.
- Decreased heat loss:
- Cutaneous vasoconstriction.
- Curling up.
- Horripilation.
Mechanisms activated by heat
- Increased heat loss:
- Cutaneous vasodilation.
- Sweating.
- Increased respiration.
- Decreased heat production:
- Anorexia.
- Apathy and inertia.
Behavioral/motor examples (explicit)
- Curling into a ball:
- Decreases body surface exposed to environment.
- Seen in animals and humans (cold bed posture).
- Cold causes:
- Shivering (involuntary skeletal muscle response).
- Semiconscious increased motor activity (foot stamping, dancing).
- Hot weather:
- Decreases activity (“too hot to move”).
Endocrine cold response details
- Increased catecholamine secretion is important in cold response.
- Knockout mice lacking dopamine β-hydroxylase (cannot make norepinephrine/epinephrine):
- Do not tolerate cold.
- Have deficient vasoconstriction.
- Cannot increase thermogenesis in brown adipose tissue via UCP1.
- TSH changes:
- Increased by cold and decreased by heat in lab animals.
- In adult humans, cold-induced TSH change is small and of questionable significance.
8) Local thermoregulatory adjustments (not just central reflexes)
- Cooling cutaneous vessels:
- Makes them more sensitive to catecholamines.
- Arterioles and venules constrict.
- Directs blood away from skin (local heat-conserving effect).
- Countercurrent heat exchange (important in cold-water mammals):
- Deep veins (venae comitantes) run alongside arteries in limbs.
- Heat transfers from warm arterial blood going to limbs to cold venous blood returning from extremities.
- Conserves body heat.
- Limits ability to maintain heat at tips of extremities.
9) Hypothalamic control centers: anterior vs posterior
- Cold-activated reflex responses are controlled from posterior hypothalamus.
- Warmth-activated reflex responses are controlled primarily from anterior hypothalamus.
- Some heat-defense persists after decerebration at rostral midbrain level.
- Effects of stimulation/lesions:
- Anterior hypothalamus stimulation:
- Cutaneous vasodilation.
- Sweating.
- Anterior hypothalamus lesions:
- Hyperthermia.
- Rectal temperatures can reach 43°C (109.4°F).
- Posterior hypothalamus stimulation:
- Shivering.
- Posterior hypothalamus lesions:
- Body temperature falls toward environmental temperature.
10) Afferent inputs integrated for temperature regulation (five sources + weighting)
- Hypothalamus integrates temperature information from:
- Skin sensory receptors (primarily cold receptors).
- Deep tissues.
- Spinal cord.
- Extrahypothalamic portions of the brain.
- Hypothalamus itself.
- Each input contributes about 20% of the integrated information.
Threshold core temperatures for key responses
- Sweating and vasodilation threshold: 37°C.
- Vasoconstriction threshold: 36.8°C.
- Nonshivering thermogenesis threshold: 36°C.
- Shivering threshold: 35.5°C.
11) Fever: thermostat reset model + mechanism chain
- Fever is a hallmark of disease and occurs in:
- Mammals, birds, reptiles, amphibia, fish.
- In homeotherms:
- Thermoregulatory mechanisms behave as if adjusted to a higher set point.
- “Thermostat reset” to above 37°C.
- Receptors signal actual temperature is below new set point.
- Temperature-raising mechanisms activate:
- Cutaneous vasoconstriction → chilly sensations.
- Sometimes shivering → shaking chill.
- Ambient temperature shapes mechanism:
- Cold environment + pyrogen: temperature rise mostly from increased heat production.
- Warm environment + pyrogen: temperature rise mostly from decreased heat loss.
Pathogenesis of fever (complete chain)
- Bacterial toxins (example: endotoxin) act on:
- Monocytes.
- Macrophages.
- Kupffer cells.
- These cells produce cytokines acting as endogenous pyrogens (EPs).
- Cytokines that can independently produce fever:
- IL-1β.
- IL-6.
- IFN-β.
- IFN-γ.
- TNF-α.
- These circulating cytokines are polypeptides and unlikely to penetrate brain.
- Evidence suggests they act on:
- OVLT (a circumventricular organ).
- OVLT activation leads to:
- Activation of preoptic area of hypothalamus.
- CNS cells can also produce cytokines in response to infection:
- These may act directly on thermoregulatory centers.
Prostaglandins as final mediator
- Fever produced by cytokines is probably due to local prostaglandin release in hypothalamus.
- Intrahypothalamic prostaglandin injection produces fever.
- Aspirin antipyretic effect:
- Exerted directly on hypothalamus.
- Inhibits prostaglandin synthesis.
- PGE2 is a prostaglandin that causes fever.
- PGE2 acts on EP receptors:
- EP1, EP2, EP3, EP4.
- EP3 receptor is critical:
- Knockout of EP3 impairs febrile response to:
- PGE2.
- IL-1β.
- Endotoxin (bacterial LPS).
Fever: benefit vs harm (as stated)
- Benefit uncertain but assumed because fever evolved and persisted.
- Reasons proposed:
- Many microbes grow best in narrow temperature range; temperature rise inhibits growth.
- Antibody production increases when body temperature is elevated.
- Historical clinical use:
- Artificial fever used for neurosyphilis before antibiotics and was beneficial.
- Hyperthermia benefits in infections listed:
- Anthrax.
- Pneumococcal pneumonia.
- Leprosy.
- Various fungal, rickettsial, and viral diseases.
- Hyperthermia slows growth of some tumors.
- Harm thresholds:
- Rectal temperature over 41°C for prolonged periods → some permanent brain damage.
- Over 43°C → heat stroke develops and death is common.
Malignant hyperthermia (mechanism)
- Caused by mutations in ryanodine receptor gene.
- Triggered by stress during muscle contraction.
- Leads to:
- Excess Ca2+ release.
- Muscle contractures.
- Increased muscle metabolism.
- Greatly increased heat production in muscle.
- Causes marked rise in body temperature fatal if not treated.
Periodic fever syndromes (genes listed + uncertainty)
- Occur with mutations in genes for:
- Pyrin (neutrophil protein).
- Mevalonate kinase (enzyme in cholesterol synthesis).
- Type 1 TNF receptor (in inflammatory responses).
- Mechanism by which these cause fever is unknown.
12) Hypothermia: hibernation, induced, and accidental
- Hibernating mammals:
- Body temperature drops to low levels during hibernation.
- No demonstrable ill effects after arousal.
- Induced hypothermia (experimental/clinical logic):
- Cooling skin or blood lowers body temperature.
- Metabolic and physiologic processes slow:
- Respiration very slow.
- Heart rate very slow.
- Blood pressure low.
- Consciousness lost.
- At rectal temperature about 28°C:
- Ability to spontaneously return temperature to normal is lost.
- Individual survives and can return to normal if externally rewarmed.
- If ice crystal formation is prevented:
- Experimental animals can be cooled to subfreezing levels without detectable damage after rewarming.
- Human tolerance:
- Humans tolerate 21–24°C (70–75°F) without permanent ill effects.
- Induced hypothermia used in surgery.
- Accidental hypothermia:
- Due to prolonged exposure to cold air or cold water.
- Serious condition requiring careful monitoring and prompt rewarming.