Big picture: what the hip bone is + why it’s built that way (logic)

- Innominate / hip bone = 3 bones fused
- Ilium + Ischium + Pubis fuse at a Y-shaped epiphysis that involves the acetabulum.
- Function logic
- Pubis + ischium together form an incomplete bony wall for the pelvic cavity
- Their outer surfaces mainly give attachment to thigh muscles.
- Ilium forms the pelvic brim between:
- hip joint (acetabulum area) and
- sacroiliac joint (joint with sacrum)
- Above the brim it becomes broad + wing-like → for ligaments + large muscles.
- Ilium thickness logic
- Anterior 2/3 of ilium = thin bone → forms iliac fossa (part of posterior abdominal wall)
- Posterior 1/3 of ilium = thick bone → carries auricular surface for sacrum + big area for strong sacroiliac ligaments that bear body weight.
- Surface logic
- Outer ilium surface → buttock muscle attachments.
- Planes (3-D orientation logic)
- Ischium + pubis lie roughly in same plane
- Ilium plane is nearly right angle to that plane.
Anatomical position checkpoints (exam positioning landmarks)



- In anatomical position:
- Pubic tubercle and ASIS are in the same vertical plane.
- Upper border of symphysis pubis and ischial spine are in the same horizontal plane.
Lateral surface: acetabulum (hip socket) logic + key facts

- Acetabulum = concave hemisphere (hip joint socket).
- Axis direction:
- Not purely horizontal
- Directed downwards + slightly backwards, along femoral neck axis.
- Inferior deficiency = acetabular notch.
- Cartilage logic (weight bearing)
- Hyaline cartilage inside acetabulum is widest over iliac part opposite the notch
- That region = main weight-bearing area.
- Articular vs non-articular
- Cartilage does NOT cover whole concavity
- Non-articular bone is thin + translucent.
- Fusion lines around acetabulum
- Pubis + ischium meet in acetabulum area; their union line continues down to the notch.
- Pubis + ilium meet at iliopubic eminence (anterior acetabular margin).
- Ilium + ischium meet at a low elevation just beyond posterior acetabular margin.

Iliac crest & vertebral level landmarks (high-yield)
- Iliac crest runs from ASIS → PSIS.
- Iliac crest tubercle
- Located 5 cm behind ASIS.
- It is the most lateral point of bony pelvis, NOT the highest point.
- Highest point of crest is 7.5 cm behind the tubercle.
- Supracristal plane
- Line joining highest points of both iliac crests passes through L4 spine.
- Tubercle vertebral level
- Iliac tubercle lies at L5 level.
Landmark | What it is / where | Vertebral level (exam) |
ASIS | Anterior end of iliac crest | L4 |
Highest point of iliac crest (Supracristal / Tuffier’s plane) | Line joining both crests | L4 spine (≈ L4–L5 space) |
Iliac tubercle | Thickened point on crest ~5 cm posterior to ASIS | L5 |
PSIS | Posterior end of iliac crest (skin dimple) | S2 |
Greater trochanter | Lateral femur, palpable | S1–S2 |

Gluteal surface: muscle attachments (exam-friendly mapping)
- 3 curved gluteal lines on gluteal surface.
- Muscle origins are separated by these lines:
- Gluteus maximus
- Gluteus medius
- Gluteus minimus
- Tensor fasciae latae (TFL)
- Origin: just below iliac crest, between ASIS and iliac tubercle.
- Rectus femoris (reflected head)
- Origin: upper margin of acetabulum.
Borders of ilium: “who attaches where” (very testable)
Anterior border (S-bend)
- ASIS:
- Inguinal ligament attaches
- Sartorius attaches
- AIIS:
- Straight head of rectus femoris attaches
- Iliofemoral ligament attaches
Posterior border
- Rounded bar between PSIS → PIIS
- Attachment: sacrotuberous ligament
- PSIS skin dimple
- PSIS makes a characteristic buttock dimple at level of 2nd piece of sacrum.(S2)
Posterior iliac crest (thicker part) attachments
- Posterior lamella of lumbar fascia attaches
- Erector spinae attaches
- Latissimus dorsi
- Aponeurotic origin fused with posterior lamella
- Additional fibres attach further forward along crest
More medial / inner side attachments on crest
- Quadratus lumborum attaches
- Iliolumbar ligament attaches
Continuing forwards on crest (abdominal wall layers)
- Internal oblique: attaches to centre of crest → up to ASIS
- Transversus abdominis: attaches to inner lip of crest → up to ASIS
- External oblique: attaches to outer lip of crest (anterior half)
Fascia lata attachment
- Attached along whole length of outer lip of iliac crest
- Splits to enclose narrow origin of TFL.
Pubis: shape, rami, crests, brim, and NV groove (full map)
- Body of pubis: quadrilateral.
- Projects laterally as:
- Superior ramus → joins ilium + ischium at acetabulum
- Inferior ramus → fuses with ischial ramus (medial to obturator foramen)
- Symphyseal surface
- Oval, coated with hyaline cartilage for secondary cartilaginous joint = pubic symphysis.
- Upper border of body = pubic crest (gently convex).
- Pubic tubercle
- Forward projecting prominence on lateral part of pubic crest.
Two ridges from pubic tubercle onto superior ramus
- Pectineal line (upper, sharp)
- Part of pelvic brim
- Joins arcuate line of ilium
- Obturator crest (lower, rounded)
- Runs down to anterior margin of acetabular notch, becomes more prominent
- Attachment: pubofemoral ligament

Between these ridges
- Surface traced laterally to the iliopubic eminence.

Pectineus + obturator groove + NV relation (very high-yield)
- Pectineus arises from pectineal line + adjacent superior ramus surface.
- Obturator groove (below obturator crest)
- Obliquely placed on pubic ramus
- Lodges obturator nerve in contact with bone
- Obturator vessels lie below the nerve as bundle passes over obturator membrane.(NAV)
Inferior ramus detail
- Marked by an everted crest.
- Junction with ischial ramus is halfway between:
- ischial tuberosity and
- pubic crest.


Pubis: abdominal wall + inguinal region + thigh adductor attachments (exam)
Pubic crest & nearby ligament/muscle attachments
- Rectus abdominis originates from pubic crest
- Pyramidalis originates in front of it
- Conjoint tendon
- Attaches to pubic crest and along pectineal line
- Lacunar ligament
- Attaches to pectineal line
- Pectineal ligament (Cooper)
- Continues along pectineal line lateral to lacunar ligament

Pubic tubercle & superficial inguinal ring relation
- Inguinal ligament attaches to pubic tubercle
- Forms lateral crus of superficial ring
- Medial crus
- In front of conjoint tendon
- Inserts into front of pubic crest alongside symphysis

Thigh muscle origins from pubis (front → downwards)
- Adductor longus: rounded tendon from front of body of pubis, in angle between pubic crest and symphysis
- Bone spurs may occur here = rider’s bone
- Gracilis: linear origin down along margin of everted crest of inferior ramus → reaches ischial ramus
- Deep to them:
- Adductor brevis from body of pubis
- Up along inferior ramus: pubic fibres of adductor magnus (deep to gracilis)
- Deeper still: obturator externus
Fascia lata (deep lamina) + perineal pouch relation
- Deep lamina attaches to pectineal line over pectineus
- Then below pubic tubercle along front of body to everted crest
- Encloses adductor longus + gracilis
- Separates them from external genitalia in superficial perineal pouch.

Teaching Script: Pubis — from Abdomen to Thigh (Exam Logic Walkthrough)
Opening framing (set the map)
“Think of the pubis as a junction bone.Above it → abdominal wall.
Medial/anterior → inguinal canal.
Below it → thigh adductors.
Superficially → perineum.
If you know what attaches where, you can predict hernias, muscle injuries, and surgical planes.”
1) Pubic crest — abdominal wall anchor point
“We start at the pubic crest, the key anchoring ridge.”
- Rectus abdominis
- Pyramidalis
- Conjoint tendon
- pubic crest
- pectineal line
→ originates from the pubic crest
→ this explains why midline abdominal tension transmits here.
→ lies in front of rectus
→ also originates from the pubic crest
→ small but exam-favourite.
→ formed by internal oblique + transversus abdominis
→ attaches to:
Exam logic:Weakening here = direct inguinal hernia risk.
2) Pectineal line — the “ligament highway”
“The pectineal line is not just bone — it’s a ligament runway.”
- Lacunar ligament
- Pectineal ligament (Cooper’s ligament)
→ attaches to the pectineal line
→ continuation along the pectineal line, lateral to lacunar ligament
→ very important surgically in hernia repair
Exam line:Cooper’s ligament = strong periosteal thickening on pectineal line.
3) Pubic tubercle — superficial inguinal ring landmark
“Shift slightly laterally to the pubic tubercle.”
- Inguinal ligament
- This attachment forms the lateral crus of the superficial inguinal ring.
- Medial crus:
- lies in front of the conjoint tendon
- inserts into front of pubic crest near the symphysis
→ attaches to the pubic tubercle
Clinical logic:Palpate pubic tubercle → you can locate the superficial inguinal ring.
4) From pubis into thigh — adductor origins (front → downwards)
“Now we drop below the pubis into the medial thigh.”
Superficial layer
- Adductor longus
- Rounded tendon
- Origin: front of body of pubis
- In the angle between pubic crest and symphysis
- Repeated stress → rider’s bone (exostosis)
- Gracilis
- Long, linear origin
- Runs down the margin of the everted crest of inferior pubic ramus
- Continues onto ischial ramus
Deep to them
- Adductor brevis
- Adductor magnus (pubic fibres)
- Obturator externus
→ from body of pubis
→ from inferior pubic ramus
→ lies deep to gracilis
→ deepest muscle here
→ arises from external surface of obturator membrane
Exam ordering rule:Front to back, superficial to deep:
Longus → Gracilis → Brevis → Magnus → Obturator externus
5) Fascia lata (deep lamina) — separating thigh from perineum
“Finally, the key surgical plane.”
- Deep lamina of fascia lata:
- Attaches to pectineal line over pectineus
- Runs below pubic tubercle
- Continues along front of pubic body
- Attaches to everted crest
- It encloses:
- Adductor longus
- Gracilis
- It separates them from:
- External genitalia
- Contents of the superficial perineal pouch
Clinical logic:Infection or hematoma in superficial perineal pouch
→ does NOT spread into thigh because of this fascial barrier.
Final exam wrap-up (one-minute recall)
“Pubic crest anchors abdominal muscles and the conjoint tendon.Pectineal line carries lacunar and Cooper’s ligaments.
Pubic tubercle marks the superficial inguinal ring.
Inferiorly, the pubis gives origin to the thigh adductors.
Fascia lata seals the thigh off from the perineum.”
Ischium: parts + sciatic notches + “who passes where” (surgery/exam)
- Ischium is L-shaped:
- Body (upper thick): joins pubis + ilium at acetabulum, extends down to ischial tuberosity → supports sitting weight
- Ramus (lower medial thin bar): joins inferior pubic ramus → encloses obturator foramen

Behind acetabulum
- Low elevation marks fusion line of ischium + ilium.
- Ischiofemoral ligament attaches at ischial margin of acetabulum.

Greater sciatic notch completion
- Upper body of ischium completes lower part of greater sciatic notch.
Sciatic nerve landmark (very testable)
- Sciatic nerve lies on ischium here, with nerve to quadratus femoris deep to it.
- Emergence point into buttock is 1/3 of the way up from ischial tuberosity → PSIS.

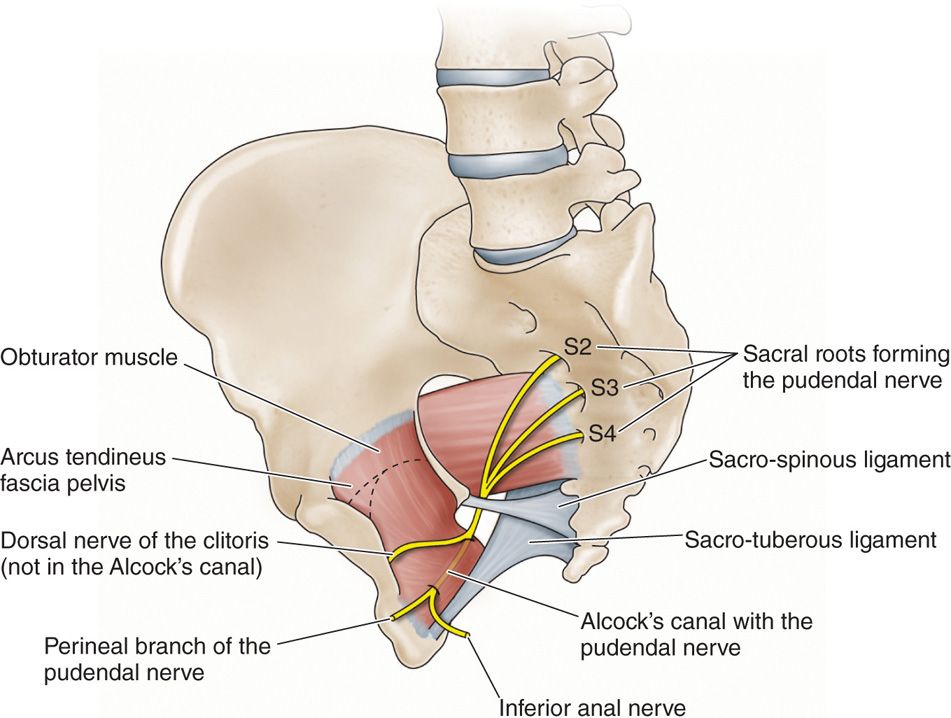
Ischial spine: key divider + key attachments + what crosses it
- Ischial spine projects medially → divides greater from lesser sciatic notch.
- Sacrospinous ligament attaches to spine → helps convert notch → greater sciatic foramen.
- Relations around spine:
- Pudendal nerve lies on sacrospinous ligament just medial to spine
- Internal pudendal vessels cross the tip
- Nerve to obturator internus lies on base
- Superior gemellus originates from the spine

Lesser sciatic notch → lesser sciatic foramen
- Lies between spine and ischial tuberosity
- Bridged by sacrotuberous ligament
- Together with sacrospinous ligament converts it to lesser sciatic foramen
- Through lesser sciatic foramen:
- Obturator internus tendon emerges into buttock
- Internal pudendal vessels + nerve pass forward into perineum
- Notch surface details:
- Grooved by tendinous fibres on deep surface of obturator internus
- Tendon separated from bone by hyaline cartilage + bursa
- Inferior gemellus originates from upper margin of ischial tuberosity (above hamstrings)

Ischium: parts + sciatic notches + “who passes where”
“The ischium is the posteroinferior weight-bearing bone of the hip, and it is the key landmark bone for understanding sciatic notches, pudendal nerve pathways, and perineal access.If you know the ischial spine, you can orient the entire pelvis surgically.”
1. Shape and parts of the ischium
“First, the basic shape.”
- The ischium is L-shaped.
- It has two main parts:
Body (upper thick part)
- Forms the posteroinferior part of the acetabulum
- Joins:
- Ilium
- Pubis
- Extends inferiorly to become the ischial tuberosity
- Functionally important:
- This is the weight-bearing bone when sitting
Exam line:“Sitting weight is transmitted through the ischial tuberosities.”
Ramus (lower thin bar)
- Runs anteromedially
- Joins the inferior pubic ramus
- Together they enclose the obturator foramen
2. Behind the acetabulum (posterior hip stability)
“Now look just behind the acetabulum.”
- A low elevation marks the fusion line of:
- Ischium
- Ilium
- This area gives attachment to the ischiofemoral ligament
Clinical relevance:This ligament is important for posterior stability of the hip joint.
3. Greater sciatic notch – how the ischium completes it
“The greater sciatic notch is not just ilium.”
- The upper body of the ischium completes the lower part of the greater sciatic notch
- When ligaments are added, this notch becomes the greater sciatic foramen
4. Sciatic nerve landmark (very high-yield)
“This is a classic exam landmark.”
- The sciatic nerve lies on the ischium at this level
- Deep to it lies the nerve to quadratus femoris
Surface landmark (must memorize)
- The sciatic nerve enters the buttock at a point:
- One-third of the way up
- From ischial tuberosity → PSIS
Exam trap:This landmark is used for safe gluteal injections and nerve blocks.
5. Ischial spine – the most important landmark
“If you remember only one structure, remember the ischial spine.”
Why it is critical
- It projects medially
- It divides:
- Greater sciatic notch (above)
- Lesser sciatic notch (below)
Attachments at the ischial spine
- Sacrospinous ligament attaches here
- Superior gemellus muscle originates from the spine
→ Converts notches into foramina
What passes in relation to the ischial spine
“This is pure exam gold — remember the relative positions.”
- Pudendal nerve
- Lies on the sacrospinous ligament
- Just medial to the spine
- Internal pudendal vessels
- Cross the tip of the spine
- Nerve to obturator internus
- Lies on the base of the spine
Mnemonic idea:Medial nerve (pudendal), tip vessels, base nerve.
6. Lesser sciatic notch → lesser sciatic foramen
“Now go below the spine.”
- The lesser sciatic notch lies:
- Between ischial spine and ischial tuberosity
- It is bridged by:
- Sacrotuberous ligament
- Sacrospinous ligament
- Together they form the lesser sciatic foramen
Structures passing through the lesser sciatic foramen
“This foramen is about turning into the perineum.”
- Obturator internus tendon
- Emerges from pelvis into buttock
- Internal pudendal vessels
- Pudendal nerve
- Pass forward to enter the perineum
Notch surface details (often ignored, but examinable)
- The inner surface of the notch is:
- Grooved by tendinous fibres of obturator internus
- The tendon is separated from bone by:
- Hyaline cartilage
- Bursa
7. Inferior gemellus origin
- Inferior gemellus originates from:
- Upper margin of the ischial tuberosity
- Above the hamstring origins
Closing exam summary (30-second recap)
“So, in summary:
- The ischium is L-shaped, weight-bearing in sitting.
- The ischial spine divides greater and lesser sciatic pathways.
- Pudendal nerve hooks around the spine.
- Obturator internus exits via the lesser sciatic foramen.
- If you know the spine, you know pelvic neurovascular surgery.”

Ischial tuberosity: surfaces + hamstrings + extra attachments
- Ischial tuberosity = rugged prominence
- Convex posterior surface divided transversely by low ridge
- Smooth oval area above ridge divided by vertical ridge into lateral + medial areas
- Semimembranosus tendon → lateral area
- Semitendinosus + long head of biceps femoris → medial area
- Between semimembranosus area and obturator foramen:
- Lateral surface gives origin to quadratus femoris
- Below transverse ridge:
- Has a longitudinal crest supporting sitting body
- Fascia lata attaches to this ridge
- Lateral bevelled surface: origin for hamstring part of adductor magnus
- Medial bevelled surface: attachment of sacrotuberous ligament
- Tuberosity curves forward into slender ischial ramus
- Adductor magnus has continuous origin along ramus for pubic part of muscle

Teaching Script: Ischial Tuberosity (Surfaces + Attachments)
“Let’s understand the ischial tuberosity logically—from shape, to surfaces, to muscle and ligament attachments.”
1. What is the ischial tuberosity? (Big picture)
- The ischial tuberosity is a large, rugged bony prominence on the inferior part of the ischium.
- It is the main weight-bearing structure during sitting.
- Because of this function, it has:
- Rough areas → muscle and ligament attachment
- Smooth areas → tendon origins
2. Posterior surface organization (key landmark)
- The posterior surface is convex.
- It is divided transversely by a low ridge into:
- Upper smooth part
- Lower rough part
This ridge is critical—everything above and below it has different functions.
3. Area ABOVE the transverse ridge (hamstrings zone)
- There is a smooth oval area.
- This oval area is divided vertically into:
- Lateral area
- Medial area
Muscle attachments (must memorize):
- Lateral area
- Medial area
→ Semimembranosus tendon
→ Semitendinosus
→ Long head of biceps femoris
Exam hook:Semimembranosus is lateral; semitendinosus + long head of biceps are medial.
4. Area between semimembranosus and obturator foramen
- The lateral surface in this region gives origin to:
- Quadratus femoris
This explains why quadratus femoris lies deep and lateral in the posterior hip region.
5. Area BELOW the transverse ridge (sitting + ligament zone)
- This part is rough and strong, designed for weight bearing.
Key features:
- A longitudinal crest:
- Supports the body during sitting
- Provides attachment to fascia lata
Bevelled surfaces:
- Lateral bevelled surface
- Origin of hamstring part of adductor magnus
- Medial bevelled surface
- Attachment of sacrotuberous ligament
Clinical logic:Sitting stresses → thick bone + ligament reinforcement on the medial side.
6. Continuation into the ischial ramus
- The ischial tuberosity curves forward to become the ischial ramus.
- Along this ramus:
- Adductor magnus has a continuous origin
- This part forms the pubic (adductor) portion of the muscle
This continuity explains why adductor magnus has both hamstring-like and adductor-like functions.
7. One-line exam summary (gold line)
“The ischial tuberosity is a weight-bearing bony prominence whose smooth upper part gives origin to hamstrings, while the rough lower part supports sitting and provides attachment to adductor magnus, fascia lata, and the sacrotuberous ligament.”
Obturator foramen + obturator membrane + obturator muscles
- Obturator foramen ringed by sharp margins of pubis + ischium
- Pubic margins overlap to form obturator groove
- Obturator membrane
- Attaches to margin of foramen
- Does NOT attach to obturator groove
- Muscle origins
- Obturator externus: outer surface of membrane + anterior bony margin of foramen
- Obturator internus: inner surface of membrane + bony margins of foramen

Teaching Script: Obturator Foramen, Membrane & Muscles
“Let’s understand this as a ring → a seal → two muscles on opposite sides.”
1️⃣ Obturator foramen — the bony ring
“First, the obturator foramen is a large opening in the hip bone.”
- It is formed by pubis + ischium
- The margins are sharp and well-defined
- Think of it as a rigid bony ring, not a soft gap
🔑 Exam lock:
Obturator foramen = pubis + ischium forming a sharp-edged ring
2️⃣ Obturator groove — the key exception
“Now, on the upper pubic part of this ring, something special happens.”
- The pubic margins overlap
- This overlap creates a small canal-like notch
- That notch is the obturator groove
⚠️ Important contrast:
- The groove is NOT part of the flat ring
- It is a channel for structures, not a surface for attachment
🔑 Exam lock:
Obturator groove is formed by overlapping pubic margins
3️⃣ Obturator membrane — the seal
“Next, the body doesn’t leave this big hole open.”
- The obturator membrane is a strong fibrous sheet
- It attaches to the margins of the obturator foramen
- It almost completely closes the foramen
🚫 Critical negative (very testable):
- The obturator membrane does NOT attach to the obturator groove
Why?
- Because the groove must stay open to form the obturator canal
🔑 Exam lock (classic MCQ):
Obturator membrane does not attach to the obturator groove
4️⃣ Obturator muscles — inside vs outside logic
“Now comes the cleanest way to remember the muscles.”
🟥 Obturator externus
- Originates from:
- Outer surface of obturator membrane
- Anterior bony margin of obturator foramen
- Located outside the pelvis
📌 Name = externus → outside
🟦 Obturator internus
- Originates from:
- Inner (pelvic) surface of obturator membrane
- Bony margins of obturator foramen
- Located inside the pelvis
📌 Name = internus → inside
5️⃣ One-line integration (final memory line)
Obturator foramen is a sharp pubis-ischium ring, sealed by the obturator membrane except at the obturator groove, with obturator internus arising from the inner surface and obturator externus from the outer surface of the membrane.
🧠 Ultra-short recall checklist (exam speed)
- Ring → pubis + ischium
- Groove → overlapping pubis
- Membrane → attaches to margins, NOT groove
- Externus → outer surface
- Internus → inner surface
Medial surface: pelvic brim, auricular surface, iliac fossa, fascia, pelvic floor anchors
Pelvic brim components (must memorize)
- Formed by:
- top of pubic crest
- pectineal line
- rounded border of ilium = arcuate line
- top of auricular surface
- Brim slopes up 60° to horizontal.
- Below brim = pelvic cavity
- Above brim = iliac fossa in abdominal cavity

Auricular area (SI joint side)
- Extends from pelvic brim to PIIS
- Surface: undulating + roughened with tubercles/depressions
- Articulates with ala of sacrum
- Anterior sacroiliac ligament attaches to sharp anterior border
Iliac fossa + iliacus
- Iliac fossa = concavity in ala of ilium in front of SI joint
- Deepest part high in fossa = paper-thin translucent bone
- Iliacus arises from upper 2/3 of this area down to level of AIIS
- Lower 1/3 separated by a large bursa from overlying iliacus
- Iliacus fibres converge and pass over broad groove between:
- iliopubic eminence and AIIS
Iliac fascia + psoas relation (clinical logic)
- Iliac fascia covers iliacus + psoas
- Attached around margins:
- iliac crest
- arcuate line
- iliopubic eminence
- Psoas major passes freely along pelvic brim and crosses iliopubic eminence deep to iliac fascia
- The “psoas bursa” deep to it is the iliacus bursa already mentioned
Pubis inner surface: pelvic floor & urogenital support
- Levator ani attaches to junction of body and inferior ramus on inner surface of pubis
- More medially:
- Puboprostatic ligaments (male) / pubovesical ligaments (female) attach at this level
- Inferior ramus lies in perineum:
- Immediately below symphyseal surface: arcuate pubic ligament attaches
- Deep dorsal vein of penis/clitoris lies in midline below it
- Along ischiopubic ramus (down from symphysis):
- Ridge for perineal membrane attachment
- External to this ridge: margin everted where:
- crus of corpus cavernosum attaches
- ischiocavernosus attaches
- Between perineal membrane and obturator foramen:
- ischiopubic ramus forms wall of anterior recess of ischioanal fossa
- Sphincter urethrae attaches here above perineal membrane
Ischium medial surface: obturator internus + pudendal canal
- Inner surface of body of ischium smooth
- Obturator internus arises from:
- body of ischium
- area above it up to arcuate line on ilium (pelvic brim)
- back to margin of greater sciatic notch
- plus obturator membrane + ischiopubic ramus

- Obturator internus fascia attaches at margins of muscle
- Fascia splits to form pudendal canal just above falciform ridge on ischial tuberosity
- Falciform ridge
- curves forward from tuberosity onto ischial ramus
- falciform process of sacrotuberous ligament attaches here

- Transverse perineal muscles attach at anterior edge of ramus
- Levator ani + coccygeus attach to inner surface of ischial spine
Medial surface of hip bone — teaching script (pelvic anatomy)
1. Pelvic brim — the boundary line (must anchor first)
“First, identify the pelvic brim.
This is the line that separates abdomen from pelvis.
It is formed sequentially by:
- the top of the pubic crest,
- the pectineal line,
- the rounded border of the ilium called the arcuate line,
- and the upper margin of the auricular surface.
The brim slopes upwards at about 60 degrees to the horizontal.
👉 Everything below this line belongs to the pelvic cavity,
👉 Everything above it is part of the iliac fossa in the abdominal cavity.
Exam anchor: Pelvic brim = pubis → pectineal line → arcuate line → auricular surface.
2. Auricular surface — sacroiliac joint side
“Now move posteriorly along the brim to the auricular area.
This surface:
- extends from the pelvic brim down to the posterior inferior iliac spine (PIIS),
- is rough and undulating, with tubercles and depressions,
- and articulates with the ala of the sacrum to form the sacroiliac joint.
Along its sharp anterior border, the anterior sacroiliac ligament attaches.
Logic: rough surface = ligament + joint stability.
3. Iliac fossa — iliacus origin zone
“Anterior to the sacroiliac joint is the iliac fossa.
This is a smooth concavity on the medial surface of the ala of the ilium.
Key points:
- The deepest part is high in the fossa, where the bone can be paper-thin and translucent.
- The iliacus muscle arises from the upper two-thirds of this fossa, extending down to the level of the AIIS.
- The lower one-third is separated from the muscle by a large iliacus bursa.
The muscle fibres converge and pass over a broad groove between:
- the iliopubic eminence, and
- the anterior inferior iliac spine (AIIS).
Clinical logic: this groove explains iliopsoas friction and bursitis.
4. Iliac fascia & psoas relationship (very testable)
“Covering both iliacus and psoas is the iliac fascia.
It attaches firmly to:
- the iliac crest,
- the arcuate line,
- and the iliopubic eminence.
Now note this carefully:
- Psoas major passes freely along the pelvic brim,
- crosses the iliopubic eminence,
- and does so deep to the iliac fascia.
The so-called psoas bursa is actually the iliacus bursa deep to the muscle.
Exam pearl: Psoas crosses the brim without attachment — explains spread of infection.
5. Pubis — pelvic floor and urogenital supports
“Shift attention to the inner surface of the pubis.
At the junction of the body and inferior ramus:
- the levator ani takes origin.
Just medial to this:
- puboprostatic ligaments in males, or
- pubovesical ligaments in females attach.
Immediately below the symphysis:
- the arcuate pubic ligament is attached,
- and in the midline beneath it lies the deep dorsal vein of the penis or clitoris.
Along the ischiopubic ramus:
- there is a ridge for perineal membrane attachment,
- lateral to this ridge the margin everts to give attachment to:
- the crus of corpus cavernosum, and
- the ischiocavernosus muscle.
Between the perineal membrane and the obturator foramen:
- the ramus forms the wall of the anterior recess of the ischioanal fossa.
Above the perineal membrane:
- the sphincter urethrae attaches here.
Logic: this area is a transition zone between pelvis, perineum, and erectile tissues.
6. Ischium (medial surface) — obturator internus & pudendal canal
“Finally, examine the medial surface of the ischium.
The inner surface of the body of the ischium is smooth and gives origin to the obturator internus.
This muscle arises from:
- the body of the ischium,
- the ilium above it up to the arcuate line,
- posteriorly up to the margin of the greater sciatic notch,
- plus the obturator membrane and ischiopubic ramus.
The obturator internus fascia attaches around the muscle margins.
Just above the falciform ridge on the ischial tuberosity:
- this fascia splits to form the pudendal canal.
The falciform ridge:
- curves forward from the tuberosity onto the ischial ramus,
- and gives attachment to the falciform process of the sacrotuberous ligament.
At the anterior edge of the ramus:
- the transverse perineal muscles attach.
On the inner surface of the ischial spine:
- the levator ani and coccygeus attach.
Exam lock: Ischial spine = landmark for pelvic floor muscles + pudendal nerve relation.
One-line wrap-up (for viva)
“The medial surface of the hip bone defines the pelvic brim, supports the sacroiliac joint, provides origin for iliacus and obturator internus, anchors the pelvic floor, and forms critical fascial pathways for the pudendal neurovascular bundle.”
Sex differences (what to look for on a dry bone)
- Female pelvis changes are mainly because:
- iliac ala is drawn out to widen pelvis
- greater sciatic notch becomes larger angle
- Key differences:
- Greater sciatic notch: near right angle in female, much less in male
- Female bone may show preauricular sulcus below arcuate line
- Ischial spine:
- Female: lies in plane of body of ischium
- Male: inverted towards pelvic cavity
- Obturator foramen:
- Female: triangular
- Male: oval
- Distance comparison:
- Pubic symphysis → anterior acetabular margin is:
- greater than acetabular diameter in female
- equal or less in male

Feature | Female Pelvis | Male Pelvis |
Greater sciatic notch | Wide, almost right angle | Narrow, much less than right angle |
Preauricular sulcus | May be present below arcuate line | Usually absent |
Ischial spine orientation | Lies in the plane of the body of ischium (less projecting) | Inverted / projects medially into pelvic cavity |
Obturator foramen shape | Triangular | Oval / round |
Distance: Pubic symphysis → anterior acetabular margin | Greater than acetabular diameter | Equal to or less than acetabular diameter |
Ossification timeline (must know ages)
- Develops in cartilage.
- 3 primary centres (near acetabulum), one for each bone:
- Ilium: appears 2nd month fetal life (weight-bearing ilium first)
- Ischium: 3rd month
- Pubis: 4th month
- At birth:
- Acetabulum is wholly cartilage
- Ilium is broad blade of bone
- Ischium + pubis are tiny bars buried in cartilage
- Growth pattern:
- 3 bones approximate each other through Y-shaped cartilage in acetabulum
- Ischial + pubic rami fuse at about 7 years
- Secondary centres appear in acetabular cartilage at 8 years
- By 18 years: ossification across acetabulum complete
- Other secondary centres around periphery fuse with main bone by 25 years
1️⃣ OBTURATOR EXTERNUS
🔹 Origin (WHY it forms a canal)
- From:
- Whole obturator membrane
- Anterior bony margin of obturator foramen
- Does NOT cover obturator notch
→ Leaves space → obturator canal
→ Passage for obturator nerve & vessels
👉 Key logic: membrane + muscle stop short superiorly → canal formation
🔹 Course (RELATION-BASED)
- Passes laterally + posteriorly
- Runs beneath femoral neck
- Narrows into a spiraling tendon
- Tendon lies in contact with posterior femoral neck
🔹 Insertion (DEEP & EXAM-FAV)
- Trochanteric fossa
- Deep pit on medial surface of greater trochanter
🔹 Hip Capsule Relation (VERY IMPORTANT)
- Posteriorly:
- Hip capsule covers ONLY half of femoral neck
- Stops where obturator externus tendon contacts periosteum
- Anteriorly:
- Capsule covers entire femoral neck
👉 Exam logic: posterior neck less intracapsular → relevance in fractures
🔹 Nerve Supply
- Posterior division of obturator nerve
- Roots: L3, L4
🔹 Action
- Lateral rotation of femur
- Dynamic stabilizer of hip (with other short rotators)
2️⃣ OBTURATOR ARTERY & NERVE – FUNCTIONAL ORGANIZATION
🔹 Obturator Artery
- Emerges via obturator canal
- Divides into:
- Anterior branch
- Posterior branch
- Both:
- Encircle obturator foramen
- Lie between obturator externus & membrane
- Anastomose with each other + medial circumflex femoral artery




🔸 Articular Branch (EXAM PEARL)
- From posterior branch
- Enters acetabular notch
- Runs in ligament of head of femur
- Supplies:
- Small area of bone near fovea capitis
👉 Key: minor but real contributor to femoral head blood supply


🔹 Obturator Nerve (L2–L4)

🔸 Division site
- Divides in obturator canal/notch into:
- Anterior division
- Posterior division
🔸 Posterior Division (DEEP & MOTOR-HEAVY)
- Passes through obturator externus
- Supplies it
- Then descends on adductor magnus
- Supplies:
- Adductor magnus
- Sometimes adductor brevis
- Terminal branch:
- Travels with femoral artery
- Through adductor hiatus
- Reaches popliteal fossa
- Supplies knee joint capsule via middle genicular artery
🔸 Anterior Division (MIXED)
- Passes above obturator externus
- Gives:
- Articular branch to hip
- Descends:
- Behind adductor longus → supplies it
- Over adductor brevis → usually supplies
- Supplies gracilis
- Ends in subsartorial plexus
- Cutaneous supply to medial thigh skin
- Direct skin branches may arise earlier
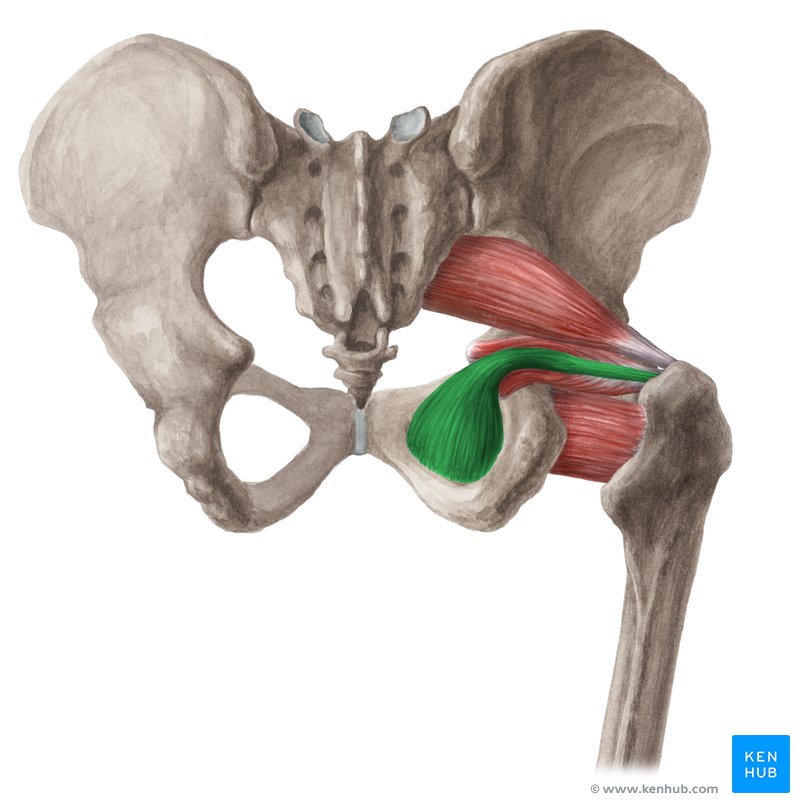
3️⃣ PIRIFORMIS – THE KEY MUSCLE
🔹 Why it is important
- Defines arrangement of gluteal neurovascular structures
🔹 Origin
- Anterior surface of middle 3 sacral segments
- Inside pelvis
- Some fibres from upper margin of greater sciatic notch
🔹 Course
- Passes posterolaterally
- Exits pelvis via greater sciatic foramen
- Almost completely fills the foramen
🔹 In Gluteal Region
- Upper border → beside gluteus medius
- Lower border → above superior gemellus
- Ends as rounded tendon
🔹 Insertion
- Medial surface of upper border of greater trochanter
🔹 Surface Anatomy (CLINICAL)
- Lower border marked by line:
- From midpoint between PSIS & coccyx
- To tip of greater trochanter
🔹 Nerve Supply
- Anterior rami of S1, S2
4️⃣ OBTURATOR INTERNUS & GEMELLI (FUNCTION AS A UNIT)
🔹 Obturator Internus
Origin
- Internal surface of lateral pelvic wall
Course
- Makes right-angled bend
- Turns around lesser sciatic notch
- Enters gluteal region
Bursa
- Tendon separated from notch by bursa
- Notch covered with hyaline cartilage
🔹 Gemelli
- Superior gemellus → upper margin of lesser sciatic notch
- Inferior gemellus → lower margin
- Reinforce obturator internus tendon
🔹 Insertion (COMMON)
- Medial surface of greater trochanter
- Above trochanteric fossa
🔹 Nerve Supply
- Nerve to obturator internus:
- L5, S1, S2
5️⃣ SUPERFICIAL CUTANEOUS NERVES OF THIGH (LOGIC MAP)
Derived from L1–L3
All supply:
- Skin
- Fascia lata
🔹 Ilioinguinal (L1)
- No lateral cutaneous branch
- Supplies:
- Root of penis
- Anterior ⅓ of scrotum
- Small medial thigh area
- Path:
- Between IO & TA
- Through superficial inguinal ring
🔹 Genitofemoral (L1–L2)
Femoral branch (L1 fibres)
- Runs on external iliac artery
- Enters femoral sheath
- Supplies skin over femoral triangle
Genital branch
- Enters spermatic cord
🔹 Medial Femoral Cutaneous (L2–L3)
- Branch of femoral nerve
- Supplies medial thigh
- Contributes to patellar plexus
🔹 Intermediate Femoral Cutaneous (L2–L3)
- Branch of femoral nerve
- Supplies front of thigh
- Also contributes to patellar plexus
🔹 Lateral Femoral Cutaneous (L2–L3)
Course
- Across iliac fossa
- Under/pierces inguinal ligament
- ~1 cm medial to ASIS
Branches
- Anterior → anterolateral thigh → patellar plexus
- Posterior → posterolateral thigh (GT → mid-thigh)
Clinical
- Compression → meralgia paraesthetica
- Pain, numbness lateral thigh
🔹 Obturator Nerve – Cutaneous
- Via subsartorial plexus
- Supplies medial thigh skin
6️⃣ FEMORAL TRIANGLE
🔹 Boundaries
- Superior → inguinal ligament
- Lateral → medial border of sartorius
- Medial → medial border of adductor longus


🔹 Floor (GUTTER-SHAPED)
- Iliacus
- Psoas
- Pectineus
- Adductor longus
🔹 Contents
- Femoral nerve
- Femoral artery
- Femoral vein
7️⃣ ILIACUS
🔹 Origin
- Iliac fossa
🔹 Course
- Passes under inguinal ligament
- Curves behind femoral vessels
- Joins psoas tendon
🔹 Insertion
- Front of psoas tendon
- Small area of femoral shaft below lesser trochanter
🔹 Bursa
- Iliopsoas (iliac) bursa
- Deep to iliacus & psoas
- Extends into upper thigh
🔹 Nerve Supply
- Femoral nerve (L2, L3)
🔹 Action
- Powerful hip flexor
- Acts with psoas major
🧠 FINAL EXAM INTEGRATION LOCK
- Obturator externus = lateral rotator + posterior capsular landmark
- Obturator nerve divisions = motor vs cutaneous logic
- Piriformis = gluteal map divider
- Obturator internus + gemelli = functional tendon unit
- Femoral triangle = surface anatomy + vascular access
- Iliacus = hip flexion powerhouse


