Hip Bone (Innominate) — SARR
Segment 1 — Big picture + 3-D orientation + anatomical position checkpoints
Q1. What is the hip bone (innominate) made of, and where do they fuse?
A
- The hip bone is made of 3 bones: ilium + ischium + pubis.
- They fuse at a Y-shaped epiphysis (triradiate cartilage) that involves the acetabulum.
- EXAM LOCK: “3 bones → triradiate (Y) cartilage → acetabulum.”
Q2. Why is the hip bone built this way (function logic)?
A
- Pubis + ischium together form an incomplete bony wall for the pelvic cavity.
- Their outer surfaces mainly provide attachment for thigh muscles.
- Ilium forms the pelvic brim link between:
- the hip joint (acetabular region) and
- the sacroiliac joint (with sacrum).
- Above the brim, the ilium becomes broad and wing-like to provide large areas for ligaments + large muscles.
- EXAM LOCK: “Pubis/ischium = pelvic wall + thigh attachments; Ilium = brim bridge (hip ↔ SI) + wing for big muscles/ligaments.”
- Clinical correlation: The ilium’s “wing” design explains why pelvis is a major muscle/ligament anchoring platform and why pelvic fractures can disrupt both load transfer and muscle forces.
Q3. Why is the ilium thin in front but thick behind?
A
- The anterior 2/3 of ilium is thin and forms the iliac fossa (part of the posterior abdominal wall).
- The posterior 1/3 of ilium is thick because it carries:
- the auricular surface (for the sacrum) and
- a large rough area for strong sacroiliac ligaments that bear body weight.
- EXAM LOCK: “Thin anterior iliac fossa; thick posterior auricular + SI ligaments = weight-bearing.”
- Clinical correlation: SI joint pain/instability tracks with the posterior 1/3 because that’s the load-bearing ligament zone.
Q4. What is the key “surface logic” of the outer ilium?
A
- The outer surface of ilium is mainly for buttock (gluteal) muscle attachments.
- EXAM LOCK: “Outer ilium = gluteal attachment surface.”
- Clinical correlation: Gluteal weakness/pain patterns often relate to pathology around lateral ilium/crest attachment regions.
Q5. How are the three bones oriented in 3-D (plane logic)?
A
- Ischium + pubis lie roughly in the same plane.
- The ilium lies in a plane that is almost at a right angle to the ischium-pubis plane.
- EXAM LOCK: “Ischiopubic plane ≈ one plane; ilium plane ≈ perpendicular.”
- Clinical correlation: This perpendicular arrangement helps create a basin + side wall architecture that resists multidirectional loads (standing, walking, sitting).
Q6. In anatomical position, what are the two key alignment checkpoints?
A
- Pubic tubercle and ASIS are in the same vertical plane.
- Upper border of symphysis pubis and ischial spine are in the same horizontal plane.
- EXAM LOCK:
- “ASIS ↕ pubic tubercle (vertical plane).”
- “Upper symphysis ↔ ischial spine (horizontal plane).”
- Clinical correlation: These checkpoints are used to confirm correct pelvic bone orientation in OSCE/dry bone stations and reduce errors when identifying ASIS/AIIS/ischial spine.
Hip Bone (Innominate) — SARR
Segment 2 — Lateral surface: acetabulum (hip socket) logic + fusion lines
Q1. What is the acetabulum (shape + role)?
A
- The acetabulum is a concave hemispherical socket for the hip joint.
- EXAM LOCK: “Acetabulum = concave hemispherical hip socket.”
- Clinical correlation: Hip stability depends on socket depth + cartilage distribution; acetabular abnormalities → instability/degeneration patterns.
Q2. What is the direction of the acetabular axis (and why does it matter)?
A
- The acetabular axis is not purely horizontal.
- It is directed downwards and slightly backwards, aligned along the axis of the femoral neck.
- EXAM LOCK: “Acetabulum faces down + slightly back → matches femoral neck axis.”
- Clinical correlation: This alignment explains why hip loading and dislocation tendencies relate to joint orientation, especially with trauma + flexion/rotation positions.
Q3. What is the inferior deficiency of the acetabulum called?
A
- The inferior deficiency is the acetabular notch.
- EXAM LOCK: “Inferior gap = acetabular notch.”
- Clinical correlation: Inferior notch region is part of the rim configuration and is relevant when thinking of rim continuity and attachment structures around the socket.
Q4. Where is acetabular hyaline cartilage thickest, and what is the logic?
A
- Hyaline cartilage inside the acetabulum is widest over the iliac part, opposite the notch.
- This corresponds to the main weight-bearing area.
- EXAM LOCK: “Widest cartilage = iliac part opposite notch = weight-bearing zone.”
- Clinical correlation: Degenerative changes and load-related pathology tend to cluster where weight-bearing cartilage is maximal.
Q5. Does cartilage cover the entire acetabular concavity?
A
- No. Cartilage does not cover the whole concavity.
- The non-articular bone is thin and translucent.
- EXAM LOCK: “Not fully cartilage-covered; non-articular bone thin/translucent.”
- Clinical correlation: Non-articular regions are not designed for load-bearing, so loading patterns are concentrated onto the articular cartilage zones.
Q6. What are the key fusion lines around the acetabulum (who meets where)?
A
- Pubis + ischium meet in the acetabular region, and their union line continues down to the acetabular notch.
- Pubis + ilium meet at the iliopubic eminence on the anterior acetabular margin.
- Ilium + ischium meet at a low elevation just beyond the posterior acetabular margin.
- EXAM LOCK (3 joins):
- “Pubis–ischium line → continues to notch.”
- “Pubis–ilium meet → iliopubic eminence (anterior margin).”
- “Ilium–ischium meet → low elevation posterior to acetabulum.”
- Clinical correlation: Acetabular fractures often propagate along bone junction lines because these represent structural transitions within the socket complex.
Hip Bone (Innominate) — SARR
Segment 3 — Iliac crest landmarks + vertebral level correlations (high-yield)
Q1. What is the iliac crest and where does it run?
A
- The iliac crest is the curved superior border of the ilium.
- It runs from ASIS → PSIS.
- EXAM LOCK: “Iliac crest = ASIS to PSIS.”
- Clinical correlation: The crest is a long palpable landmark used for surface anatomy, injections, and incision planning.
Q2. What is the iliac crest tubercle (location + significance)?
A
- The iliac tubercle lies ~5 cm behind the ASIS.
- It is the most lateral point of the bony pelvis.
- It is NOT the highest point of the crest.
- EXAM LOCK: “Tubercle = 5 cm behind ASIS; most lateral, not highest.”
- Clinical correlation: Lateral pelvic width assessments and belt-line palpation often identify the tubercle, not the crest’s summit.
Q3. Where is the highest point of the iliac crest?
A
- The highest point of the iliac crest lies ~7.5 cm behind the iliac tubercle.
- EXAM LOCK: “Highest crest point = 7.5 cm behind tubercle.”
- Clinical correlation: This point is used to define the supracristal plane.
Q4. What is the supracristal plane and which vertebral level does it cross?
A
- The supracristal plane is a line joining the highest points of both iliac crests.
- It passes through the L4 vertebral spine.
- EXAM LOCK: “Supracristal plane → L4.”
- Clinical correlation: Lumbar puncture level estimation and spinal landmarking rely on L4 via the crest.
Q5. Which vertebral level corresponds to the iliac tubercle?
A
- The iliac tubercle lies at the L5 vertebral level.
- EXAM LOCK: “Iliac tubercle → L5.”
- Clinical correlation: Differentiating L4 (crest high point) from L5 (tubercle) prevents common exam and procedural errors.
Reply “next” for Segment 4 (Gluteal surface: gluteal lines + muscle origins, including TFL and rectus femoris).
Hip Bone (Innominate) — SARR
Segment 4 — Gluteal surface: gluteal lines + muscle origins (exam-friendly map)

Q1. What defines the gluteal surface of the ilium?
A
- The gluteal surface is the outer surface of the ilium.
- It is marked by three curved gluteal lines.
- These lines partition muscle origins.
- EXAM LOCK: “3 curved gluteal lines = muscle origin boundaries.”
- Clinical correlation: Pain/weakness patterns in the buttock often map directly to which gluteal line zone is involved.
Q2. Which muscles originate in relation to the gluteal lines?
A
- The three gluteal muscles arise from areas separated by the three gluteal lines:
- Gluteus maximus
- Gluteus medius
- Gluteus minimus
- EXAM LOCK: “Each gluteal muscle has its own gluteal-line zone.”
- Clinical correlation:
- Medius/minimus pathology → Trendelenburg gait.
- Maximus pathology → difficulty rising/climbing.
Q3. Where does tensor fasciae latae (TFL) originate?
A
- TFL originates from:
- Just below the iliac crest
- Between ASIS and the iliac tubercle
- EXAM LOCK: “TFL = below crest, ASIS ↔ tubercle.”
- Clinical correlation: Tight TFL contributes to IT band syndrome and lateral hip pain.
Q4. Where does rectus femoris arise on the lateral hip bone?
A
- The reflected head of rectus femoris arises from the upper margin of the acetabulum.
- EXAM LOCK: “Rectus femoris (reflected head) = acetabular margin.”
- Clinical correlation: Anterior hip pain after kicking/sprinting can involve acetabular margin traction via rectus femoris.
Reply “next” for Segment 5 (Borders of the ilium — anterior/posterior borders + ligament and muscle attachments).
Hip Bone (Innominate) — SARR
Segment 5 — Borders of the ilium: “who attaches where” (very testable)
Q1. What characterises the anterior border of the ilium?
A
- The anterior border has an S-shaped bend.
- It bears two key spines:
- ASIS
- AIIS
- EXAM LOCK: “Anterior border = S-bend with ASIS + AIIS.”
- Clinical correlation: These spines are frequent sites of avulsion injuries in athletes and landmarks for inguinal region surgery.
Q2. What attaches to the ASIS?
A
- Inguinal ligament
- Sartorius muscle
- EXAM LOCK: “ASIS → inguinal ligament + sartorius.”
- Clinical correlation: Pain near ASIS after sprinting can indicate sartorius strain; inguinal ligament anchoring explains groin pain patterns.
Q3. What attaches to the AIIS?
A
- Straight head of rectus femoris
- Iliofemoral ligament
- EXAM LOCK: “AIIS → rectus femoris (straight head) + iliofemoral ligament.”
- Clinical correlation: Kicking injuries often involve AIIS avulsion via rectus femoris traction.
Q4. What defines the posterior border of the ilium?
A
- A rounded bar extending from PSIS → PIIS.
- Sacrotuberous ligament attaches along this border.
- EXAM LOCK: “Posterior border PSIS→PIIS = sacrotuberous ligament.”
- Clinical correlation: Posterior pelvic pain and stability issues relate to sacrotuberous ligament tension.
Q5. Why is PSIS clinically recognisable on the surface?
A
- PSIS produces a characteristic skin dimple.
- This dimple lies at the level of the 2nd piece of the sacrum.
- EXAM LOCK: “PSIS dimple → S2 level.”
- Clinical correlation: Surface landmarking for SI joint assessment and injections uses the PSIS dimple.
Q6. What attaches to the posterior iliac crest (thicker part)?
A
- Posterior lamella of lumbar fascia
- Erector spinae
- Latissimus dorsi
- Aponeurotic origin fused with posterior lamella
- Additional fibres extend further forward along the crest
- EXAM LOCK: “Posterior crest → lumbar fascia, erector spinae, latissimus dorsi.”
- Clinical correlation: Low back pain syndromes often involve this myofascial anchoring zone.
Q7. What attaches to the medial/inner side of the iliac crest?
A
- Quadratus lumborum
- Iliolumbar ligament
- EXAM LOCK: “Medial crest → QL + iliolumbar ligament.”
- Clinical correlation: Iliolumbar ligament strain can mimic L5 radiculopathy.
Q8. How do the abdominal wall muscles attach along the crest (anterior half)?
A
- Internal oblique → attaches to the centre of the crest up to ASIS
- Transversus abdominis → attaches to the inner lip up to ASIS
- External oblique → attaches to the outer lip of the anterior half
- EXAM LOCK:
- “IO = centre”
- “TA = inner lip”
- “EO = outer lip (anterior half)”
- Clinical correlation: Abdominal wall weakness and sports hernia patterns track to these layered attachments.
Q9. Where does the fascia lata attach on the ilium?
A
- Along the entire length of the outer lip of the iliac crest.
- It splits to enclose the narrow origin of tensor fasciae latae.
- EXAM LOCK: “Fascia lata = whole outer lip; splits around TFL.”
- Clinical correlation: This explains tension transmission from TFL → IT band → lateral knee pain.
Hip Bone (Innominate) — SARR
Segment 6 — Pubis: body, rami, crests, ridges & obturator NV logic (very high-yield)



Q1. What is the basic shape of the pubis and how does it project?
A
- The body of pubis is quadrilateral.
- It projects laterally as:
- Superior ramus → joins ilium + ischium at the acetabulum
- Inferior ramus → fuses with ischial ramus medial to the obturator foramen
- EXAM LOCK: “Pubis body quadrilateral; superior ramus → acetabulum; inferior ramus → ischial ramus.”
- Clinical correlation: Fractures follow rami; superior ramus fractures affect pelvic brim/acetabular relations, inferior ramus fractures affect perineal mechanics.
Q2. What is the symphyseal surface and what joint does it form?
A
- The symphyseal surface is oval and coated with hyaline cartilage.
- It forms a secondary cartilaginous joint → pubic symphysis.
- EXAM LOCK: “Pubic symphysis = secondary cartilaginous joint with hyaline cartilage.”
- Clinical correlation: Pregnancy and trauma widen/strain this joint → symphysis pain/instability.
Q3. What are the pubic crest and pubic tubercle?
A
- The upper border of the pubic body is the pubic crest (gently convex).
- The pubic tubercle is a forward-projecting prominence on the lateral part of the crest.
- EXAM LOCK: “Crest = upper border; tubercle = forward projection laterally.”
- Clinical correlation: The tubercle is a palpable landmark for inguinal surgery.
Q4. What are the two ridges running from the pubic tubercle onto the superior ramus?
A
- Pectineal line (upper, sharp)
- Part of the pelvic brim
- Continuous with the arcuate line of ilium
- Obturator crest (lower, rounded)
- Runs toward the anterior margin of the acetabular notch
- Becomes more prominent laterally
- Attachment for pubofemoral ligament
- EXAM LOCK:
- “Pectineal line = pelvic brim.”
- “Obturator crest = pubofemoral ligament.”
- Clinical correlation: Surgical fixation or sutures here risk muscle, ligament, and NV structures.
Q5. What lies between these two ridges?
A
- The surface between the pectineal line and obturator crest traces laterally to the iliopubic eminence.
- EXAM LOCK: “Between ridges → iliopubic eminence corridor.”
- Clinical correlation: This corridor is crossed in femoral hernia repair, explaining risk to obturator structures.
Q6. Where does pectineus arise and why is it tested?
A
- Pectineus arises from the pectineal line and adjacent superior ramus surface.
- EXAM LOCK: “Pectineus ← pectineal line.”
- Clinical correlation: Injury causes pain on hip flexion + adduction; common in groin strain patterns.
Q7. What is the obturator groove and what passes through it (order matters)?
A
- The obturator groove lies below the obturator crest on the superior pubic ramus.
- It is obliquely placed.
- Contents (VERY HIGH-YIELD order):
- Obturator nerve → in contact with bone
- Obturator vessels → below the nerve as a bundle
- EXAM LOCK: “Nerve on bone; vessels below.”
- Clinical correlation:
- Medial thigh pain = obturator nerve irritation
- Bleeding = obturator vessels
- The nerve is injured first because it lies directly on bone.
Q8. What are the key features of the inferior pubic ramus?
A
- Marked by an everted crest.
- Fuses with the ischial ramus.
- The junction lies halfway between:
- the ischial tuberosity and
- the pubic crest
- EXAM LOCK: “Inferior ramus everted crest; junction midway tuberosity ↔ crest.”
- Clinical correlation: Fractures here disrupt pelvic ring stability, perineal membrane, and adductor origins.
Reply “next” for Segment 7 (Pubis in surgery: femoral hernia corridor, corona mortis risk, obturator pain logic).
Hip Bone (Innominate) — SARR
Segment 7 — Pubis in surgery: femoral hernia corridor, corona mortis, obturator pain logic




Q1. Why is the pubis inevitably encountered in femoral hernia repair?
A
- The body of pubis forms the anterior wall of the pelvis.
- Dissection near the femoral ring brings the surgeon onto:
- Pubic crest
- Pubic tubercle
- Superior pubic ramus
- EXAM LOCK: “Femoral hernia → pubic tubercle + superior ramus.”
- Clinical correlation: The pubic tubercle is the surface landmark guiding incision placement.
Q2. How do the pubic crest and pubic tubercle create a surgical danger zone?
A
- The pubic crest is the upper border of the pubic body.
- The pubic tubercle projects forward and gives rise to two ridges on the superior ramus.
- These ridges define where mesh, sutures, and dissection commonly pass.
- EXAM LOCK: “Crest → tubercle → two ridges = danger lines.”
- Clinical correlation: Misplaced sutures here risk bleeding + nerve pain.
Q3. What is the upper ridge and why is it risky?
A
- The upper ridge is the pectineal line.
- It forms part of the pelvic brim and continues laterally as the arcuate line.
- EXAM LOCK: “Pectineal line = pelvic brim.”
- Clinical correlation:
- Fixation here risks pectineus (origin)
- Pain on hip flexion/adduction may follow.
Q4. What is the lower ridge and why is it risky?
A
- The lower ridge is the obturator crest.
- It runs toward the anterior margin of the acetabular notch.
- It gives attachment to the pubofemoral ligament.
- EXAM LOCK: “Obturator crest → pubofemoral ligament.”
- Clinical correlation: Dissection too deep/medial here endangers obturator canal contents.
Q5. What lies between the two ridges—and why does it matter most?
A
- The surface between the pectineal line and obturator crest leads to the iliopubic eminence.
- This is the exact corridor crossed in femoral hernia repair.
- EXAM LOCK: “Between ridges = iliopubic corridor.”
- Clinical correlation: This is where corona mortis variants may cross.
Q6. What is corona mortis (and why surgeons fear it)?
A
- Corona mortis is a vascular variant where:
- An aberrant obturator vessel (artery ± vein) connects with external iliac or inferior epigastric vessels.
- It often crosses the superior pubic ramus near the pectineal line.
- EXAM LOCK: “Corona mortis = aberrant obturator vessel over superior pubic ramus.”
- Clinical correlation:
- Injury → brisk, hard-to-control bleeding
- Bleeding occurs because the vessel is unexpected + tethered to bone.
Q7. Where is the obturator groove, and what is the exact NV order?
A
- The obturator groove lies below the obturator crest on the superior pubic ramus.
- It is obliquely placed.
- Contents (order is critical):
- Obturator nerve → directly on bone
- Obturator vessels → below the nerve
- EXAM LOCK: “Nerve on bone; vessels below.”
- Clinical correlation:
- Medial thigh pain → obturator nerve irritation
- Bleeding → obturator vessels
- The nerve is injured first because it lies against bone.
Q8. How does this anatomy explain post-op medial thigh pain?
A
- Surgical traction/edema near the obturator groove irritates the obturator nerve.
- The nerve supplies medial thigh sensation and adductor function.
- EXAM LOCK: “Medial thigh pain post-op = obturator nerve.”
- Clinical correlation: Difficulty with adduction may accompany sensory pain.
Q9. Why might pectineus pain coexist after surgery?
A
- Pectineus originates from the pectineal line.
- Fixation or inflammation at the brim irritates this origin.
- EXAM LOCK: “Pectineus ← pectineal line.”
- Clinical correlation: Pain with hip flexion/adduction points to pectineus involvement.
Reply “next” for Segment 8 (Pubis: abdominal wall, inguinal region, and thigh adductor attachments—exam synthesis).
Hip Bone (Innominate) — SARR
Segment 8 — Pubis: abdominal wall, inguinal region & thigh adductor attachments (exam synthesis)




Q1. Which abdominal wall structures attach to the pubic crest?
A
- Rectus abdominis originates from the pubic crest.
- Pyramidalis arises in front of rectus abdominis from the pubic crest.
- Conjoint tendon attaches to:
- Pubic crest
- Along the pectineal line
- EXAM LOCK: “Pubic crest → rectus abdominis, pyramidalis, conjoint tendon.”
- Clinical correlation: Repetitive strain here → sports hernia / inguinal disruption.
Q2. What ligaments attach along the pectineal line in the inguinal region?
A
- Lacunar ligament attaches to the pectineal line.
- Pectineal ligament (Cooper’s) continues laterally along the pectineal line beyond the lacunar ligament.
- EXAM LOCK: “Pectineal line → lacunar + Cooper’s ligament.”
- Clinical correlation: Mesh fixation during hernia repair often anchors to Cooper’s ligament.
Q3. How is the pubic tubercle related to the superficial inguinal ring?
A
- Inguinal ligament attaches to the pubic tubercle.
- It forms the lateral crus of the superficial inguinal ring.
- The medial crus:
- Inserts into the front of the pubic crest
- Lies in front of the conjoint tendon
- EXAM LOCK: “Pubic tubercle = inguinal ligament = lateral crus.”
- Clinical correlation: Pain/bulge near the tubercle ≠ testicular pathology by default.
Q4. Which thigh muscles arise from the pubis (front → downwards)?
A
- Adductor longus
- Rounded tendon from the front of pubic body
- In the angle between pubic crest and symphysis
- Chronic traction → rider’s bone
- Gracilis
- Linear origin along the everted crest of inferior pubic ramus
- Continues to ischial ramus
- EXAM LOCK: “Adductor longus (front of body); Gracilis (inferior ramus everted crest).”
- Clinical correlation: Groin strains often localize to adductor longus origin.
Q5. Which deep muscles arise from the pubis/inferior ramus?
A
- Adductor brevis → from body of pubis (deep to adductor longus)
- Pubic fibres of adductor magnus → from inferior ramus (deep to gracilis)
- Obturator externus → deepest, from outer surface of obturator membrane + bony margins
- EXAM LOCK: “Brevis (body), Magnus pubic fibres (inferior ramus), Obturator externus (deepest).”
- Clinical correlation: Deep groin pain with resisted external rotation → obturator externus.
Q6. Where does the fascia lata (deep lamina) attach, and why does it matter?
A
- Attaches to the pectineal line over pectineus.
- Continues below the pubic tubercle along the front of the pubic body to the everted crest.
- Encloses adductor longus + gracilis.
- Separates them from the superficial perineal pouch & external genitalia.
- EXAM LOCK: “Deep fascia lata → pectineal line; encloses adductors; spares genitalia.”
- Clinical correlation: Deep groin pain without scrotal/penile swelling localizes to pubic/adductor pathology.
Q7. Integrated exam pattern — how do these attachments explain common symptom clusters?
A
- Groin pain + cough pain → pubic crest + conjoint tendon
- Pain near pubic tubercle → inguinal ligament attachment
- Medial thigh pain → adductor longus/gracilis origins
- No genital swelling → fascia lata barrier intact
- EXAM LOCK: “One pubic bone → abdominal wall + inguinal + adductors = mixed groin syndromes.”
Reply “next” for Segment 9 (Ischium: parts, sciatic notches, ischial spine, and who passes where).
Hip Bone (Innominate) — SARR
Segment 9 — Ischium: parts, sciatic notches, ischial spine, and “who passes where” (surgery + exam)




Q1. What are the parts of the ischium, and why is it L-shaped?
A
- The ischium is L-shaped with:
- Body (upper, thick)
- Joins pubis + ilium at the acetabulum
- Extends down to the ischial tuberosity
- Bears sitting weight
- Ramus (lower, thin, medial bar)
- Joins inferior pubic ramus
- Helps enclose the obturator foramen
- EXAM LOCK: “Ischium = thick body (sitting weight) + thin ramus (obturator ring).”
- Clinical correlation: Pain on sitting → suspect ischial body/tuberosity involvement.
Q2. What landmark lies behind the acetabulum on the ischium?
A
- A low elevation marks the fusion line of ischium + ilium.
- The ischiofemoral ligament attaches at the ischial margin of the acetabulum.
- EXAM LOCK: “Posterior acetabular margin → ischiofemoral ligament.”
- Clinical correlation: Posterior hip pain with extension/external rotation can involve this ligament.
Q3. How does the ischium contribute to the greater sciatic notch?
A
- The upper body of the ischium completes the lower part of the greater sciatic notch.
- EXAM LOCK: “Ischial body completes greater sciatic notch.”
- Clinical correlation: Notch-to-foramen conversion is crucial for neurovascular passage.
Q4. Where is the sciatic nerve in relation to the ischium (key landmark)?
A
- The sciatic nerve lies on the ischium just behind the acetabulum.
- It emerges into the buttock at a point 1/3 of the distance from the ischial tuberosity to the PSIS.
- The nerve to quadratus femoris lies deep to the sciatic nerve here.
- EXAM LOCK: “Sciatic nerve exit = 1/3 up from tuberosity → PSIS.”
- Clinical correlation: Posterior acetabular fixation or swelling here → sciatica.
Q5. What is the ischial spine, and why is it a divider?
A
- The ischial spine projects medially.
- It divides the:
- Greater sciatic notch (above)
- Lesser sciatic notch (below)
- EXAM LOCK: “Ischial spine = divider of sciatic notches.”
- Clinical correlation: Landmark for pudendal nerve block.
Q6. Which ligament attaches to the ischial spine, and what does it create?
A
- Sacrospinous ligament attaches to the ischial spine.
- It helps convert the greater sciatic notch → greater sciatic foramen.
- EXAM LOCK: “Sacrospinous ligament → greater sciatic foramen.”
- Clinical correlation: Injury here destabilizes pelvic outlet and risks nerve compression.
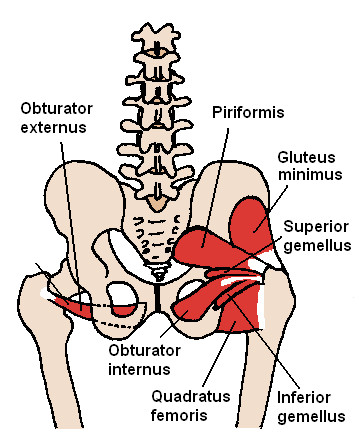
Q7. What structures pass around the ischial spine (order matters)?
A
- Pudendal nerve → lies on the sacrospinous ligament just medial to the spine
- Internal pudendal vessels → cross the tip of the spine
- Nerve to obturator internus → lies at the base of the spine
- Superior gemellus → originates from the spine
- EXAM LOCK:
- “Pudendal nerve = medial”
- “Vessels = tip”
- “Nerve to OI = base”
- Clinical correlation: Compression here → perineal numbness ± sphincter symptoms.
Q8. What is the lesser sciatic notch, and how does it become a foramen?
A
- The lesser sciatic notch lies between:
- Ischial spine (above)
- Ischial tuberosity (below)
- It is converted into the lesser sciatic foramen by:
- Sacrospinous ligament
- Sacrotuberous ligament
- EXAM LOCK: “Two ligaments → lesser sciatic foramen.”
- Clinical correlation: Entrapment here → deep buttock pain with hip rotation.
Q9. What passes through the lesser sciatic foramen?
A
- Obturator internus tendon (exits pelvis)
- Internal pudendal vessels + pudendal nerve (re-enter perineum)
- EXAM LOCK: “OI tendon out; pudendal bundle forward to perineum.”
- Clinical correlation: Pain with hip rotation + perineal symptoms → think lesser sciatic foramen.
Q10. What are the surface details of the lesser sciatic notch?
A
- The notch surface is grooved by the tendinous fibres of obturator internus.
- The tendon is separated from bone by hyaline cartilage + a bursa.
- Inferior gemellus arises from the upper margin of the ischial tuberosity (just below).
- EXAM LOCK: “OI tendon groove + cartilage + bursa; inferior gemellus below.”
- Clinical correlation: Bursitis here mimics piriformis-type deep buttock pain.
Reply “next” for Segment 10 (Ischial tuberosity: surfaces, hamstring origins, sacrotuberous ligament, and sitting pain logic).
Hip Bone (Innominate) — SARR
Segment 10 — Ischial tuberosity: surfaces, hamstrings, ligament anchors & sitting-pain logic




Q1. What is the ischial tuberosity, and why is it clinically important?
A
- The ischial tuberosity is a rugged prominence at the inferior end of the ischial body.
- It is the primary weight-bearing point in sitting.
- EXAM LOCK: “Pain on sitting → ischial tuberosity.”
- Clinical correlation: Sitting intolerance, bursitis, and proximal hamstring problems localize here.
Q2. How is the posterior surface of the tuberosity organised?
A
- The posterior surface is convex.
- It is divided transversely by a low ridge.
- EXAM LOCK: “Posterior tuberosity = convex + transverse ridge.”
- Clinical correlation: Pressure over this ridge explains sitting pain on hard surfaces.
Q3. What is found above the transverse ridge (smooth oval area)?
A
- A smooth oval area divided by a vertical ridge into:
- Lateral area → Semimembranosus tendon
- Medial area → Semitendinosus + long head of biceps femoris
- EXAM LOCK:
- “Semimembranosus = lateral.”
- “Semitendinosus + BFLH = medial.”
- Clinical correlation: Pain on hip flexion + knee extension points to proximal hamstring origin pathology.
Q4. What lies between the semimembranosus area and the obturator foramen?
A
- The lateral surface here gives origin to quadratus femoris.
- EXAM LOCK: “Quadratus femoris → lateral surface near obturator foramen.”
- Clinical correlation: Deep buttock pain worsened by external rotation implicates quadratus femoris.
Q5. What structures attach below the transverse ridge?
A
- A longitudinal crest that supports sitting body weight.
- Fascia lata attaches to this crest.
- EXAM LOCK: “Below ridge = longitudinal crest + fascia lata.”
- Clinical correlation: Fascial tension contributes to posterior thigh discomfort with prolonged sitting.
Q6. What attaches to the bevelled surfaces below the ridge?
A
- Lateral bevelled surface → Hamstring (ischial) part of adductor magnus
- Medial bevelled surface → Sacrotuberous ligament
- EXAM LOCK:
- “Lateral bevel → adductor magnus (hamstring part).”
- “Medial bevel → sacrotuberous ligament.”
- Clinical correlation:
- Weak hip extension → adductor magnus involvement
- Medial pelvic pull → sacrotuberous ligament strain
Q7. How does the tuberosity continue inferiorly?
A
- It curves forward into the slender ischial ramus.
- Adductor magnus has a continuous origin along the ramus for its pubic part.
- EXAM LOCK: “Tuberosity → ramus → adductor magnus continuity.”
- Clinical correlation: Combined weakness in hip extension + adduction fits adductor magnus origin spread.
Q8. Integrated pattern recognition — how do symptoms map to attachments?
A
- Sitting pain → transverse ridge + longitudinal crest
- Pain with hamstring stretch → semimembranosus / semitendinosus / biceps femoris origins
- Deep buttock pain with ER → quadratus femoris
- Medial pelvic pull → sacrotuberous ligament
- Hip extension weakness → adductor magnus (ischial part)
- EXAM LOCK: “One tuberosity → multiple pain generators.”
Reply “next” for Segment 11 (Obturator foramen, obturator membrane, obturator internus vs externus—deep hip pain logic).
Hip Bone (Innominate) — SARR
Segment 11 — Obturator foramen + obturator membrane + obturator muscles (deep hip pain logic)


Q1. What forms the obturator foramen, and why is it almost closed?
A
- The obturator foramen is formed by the pubis + ischium.
- It is almost completely closed by the obturator membrane.
- EXAM LOCK: “Pubis + ischium → obturator foramen; membrane closes it.”
- Clinical correlation: Large bony opening converted into a stability plate for muscle anchoring.
Q2. What is special about the obturator groove?
A
- The obturator groove is formed by overlapping pubic margins.
- The obturator membrane does NOT attach to the groove.
- This leaves a canal.
- EXAM LOCK: “Membrane spares groove → obturator canal.”
- Clinical correlation: This is the only exit for obturator NV structures.
Q3. What passes through the obturator canal (order matters)?
A
- Obturator nerve
- Obturator artery
- Obturator vein
- EXAM LOCK: “Obturator canal → nerve + vessels.”
- Clinical correlation: Obturator hernia or surgery → medial thigh pain + adductor weakness (Howship–Romberg).
Q4. Where does obturator externus arise, and what does it do?
A
- Origin:
- Outer surface of obturator membrane
- Anterior bony margin of obturator foramen
- Action:
- External rotation of hip
- Stabilises femoral head
- EXAM LOCK: “Externus = outer membrane + anterior margin; ER stabiliser.”
- Clinical correlation: Pain on resisted external rotation with deep anterior hip pain → externus strain.
Q5. Where does obturator internus arise, and why is it prone to pain?
A
- Origin:
- Inner surface of obturator membrane
- Bony margins of obturator foramen
- Body of ischium
- Pelvic surface of ilium up to the arcuate line
- Margin of greater sciatic notch
- Course:
- Turns sharply around the lesser sciatic notch
- Action:
- External rotation (hip extended)
- Abduction (hip flexed)
- EXAM LOCK: “Internus = inner membrane + pelvic walls; sharp turn at lesser sciatic notch.”
- Clinical correlation: Spasm/inflammation → deep pelvic or posterior hip pain, worse with sitting or rotation.
Q6. Why does obturator internus pain feel “deep” rather than superficial?
A
- The muscle arises from the pelvic surface.
- It is covered by obturator internus fascia.
- EXAM LOCK: “Pelvic origin = deep pain.”
- Clinical correlation: Mimics piriformis syndrome but lies deeper and more medial.
Q7. Key surgical rule to remember?
A
- The obturator membrane never closes the obturator canal.
- EXAM LOCK: “Groove always open → NV risk.”
- Clinical correlation: Pelvic surgery near the superior pubic ramus must anticipate obturator NV injury.
Reply “next” for Segment 12 (Medial surface: pelvic brim, auricular surface, iliac fossa, iliacus–psoas–fascia logic).
Hip Bone (Innominate) — SARR
Segment 12 — Medial surface: pelvic brim, auricular surface, iliac fossa & iliacus–psoas–fascia logic




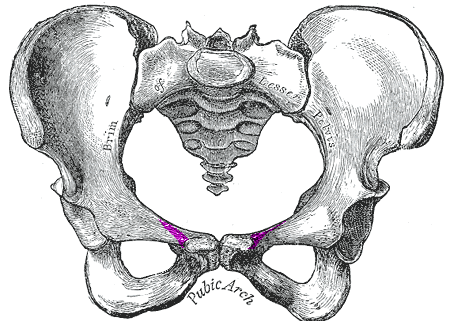
Q1. What structures together form the pelvic brim (must list in order)?
A
- Top of pubic crest
- Pectineal line
- Arcuate line of ilium (rounded medial border)
- Upper margin of auricular surface
- EXAM LOCK: “Pubic crest → pectineal line → arcuate line → auricular margin = pelvic brim.”
- Clinical correlation: Fracture lines and force transmission often track along the brim.
Q2. What is the orientation of the pelvic brim and why does it matter?
A
- The brim slopes ~60° upward from anterior to posterior.
- Below the brim lies the pelvic cavity.
- Above the brim lies the iliac fossa (abdominal cavity).
- EXAM LOCK: “60° slope; below = pelvis, above = abdomen.”
- Clinical correlation: Explains why some pelvic injuries spare abdominal contents but cause pelvic organ symptoms.
Q3. What is the auricular surface and what attaches here?
A
- The auricular surface is an undulating, roughened area on the medial ilium.
- It extends from the pelvic brim down to the PIIS.
- It articulates with the ala of the sacrum (SI joint).
- The anterior sacroiliac ligament attaches to its sharp anterior border.
- EXAM LOCK: “Auricular surface → SI joint; anterior SI ligament on sharp border.”
- Clinical correlation: SI joint pain localises to this posteromedial ilium.
Q4. What is the iliac fossa, and why is its bone sometimes translucent?
A
- The iliac fossa is the concavity of the ala of ilium anterior to the SI joint.
- The deepest part (high in the fossa) has paper-thin, translucent bone.
- EXAM LOCK: “Iliac fossa thin anteriorly.”
- Clinical correlation: Force transmission here can irritate iliacus and produce hip-flexion pain.
Q5. Where does iliacus arise and how do its fibres course?
A
- Iliacus arises from the upper 2/3 of the iliac fossa down to the AIIS.
- The lower 1/3 is separated from bone by a large iliacus bursa.
- Fibres converge and pass over a broad groove between AIIS and iliopubic eminence.
- EXAM LOCK: “Iliacus = upper 2/3 fossa; bursa below; groove AIIS ↔ iliopubic eminence.”
- Clinical correlation: Rising from supine and resisted hip flexion aggravate iliacus/bursa pain.
Q6. What is the iliac fascia, and where does it attach?
A
- The iliac fascia covers iliacus + psoas.
- It attaches firmly to:
- Iliac crest
- Arcuate line
- Iliopubic eminence
- EXAM LOCK: “Iliac fascia anchors at crest, arcuate line, iliopubic eminence.”
- Clinical correlation: Fascial continuity explains spread of inflammation between iliacus ↔ psoas.
Q7. How does psoas major relate to the brim and fascia (key insight)?
A
- Psoas major passes freely along the pelvic brim.
- It crosses the iliopubic eminence deep to the iliac fascia.
- The so-called “psoas bursa” here is actually the iliacus bursa.
- EXAM LOCK: “Psoas crosses brim deep to fascia; ‘psoas bursa’ = iliacus bursa.”
- Clinical correlation: Iliacus inflammation often refers pain along psoas into the lumbar region/anterior thigh.
Reply “next” for Segment 13 (Pubis inner surface & perineum: pelvic floor anchors, perineal membrane, pudendal canal relations).
Hip Bone (Innominate) — SARR
Segment 13 — Pubis inner surface & perineum: pelvic floor anchors, perineal membrane, pudendal relations


Q1. Where does the pelvic floor (levator ani) attach on the pubis?
A
- Levator ani attaches to the junction of the body of pubis and the inferior pubic ramus on the inner surface.
- EXAM LOCK: “Levator ani → body–inferior ramus junction (inner pubis).”
- Clinical correlation: Fracture or strain here → pelvic floor pain/weakness, pain on attempted contraction.
Q2. What urogenital support ligaments attach medially on the inner pubis?
A
- Puboprostatic ligaments (male) / Pubovesical ligaments (female) attach medially on the inner pubic surface.
- EXAM LOCK: “Inner pubis → bladder/prostate support ligaments.”
- Clinical correlation: Injury → urinary discomfort, pelvic heaviness.
Q3. What attaches immediately below the symphyseal surface?
A
- The arcuate pubic ligament attaches just below the symphysis.
- The deep dorsal vein of penis/clitoris runs in the midline immediately below this ligament.
- EXAM LOCK: “Arcuate pubic ligament above; deep dorsal vein just below.”
- Clinical correlation: Perineal bruising or erectile discomfort after trauma localizes to this midline zone.
Q4. How does the ischiopubic ramus anchor the perineal membrane?
A
- Along the ischiopubic ramus there is a ridge for perineal membrane attachment.
- External to this ridge (everted margin):
- Crus of corpus cavernosum
- Ischiocavernosus muscle
- EXAM LOCK: “Ridge = perineal membrane; outside ridge = erectile tissue + ischiocavernosus.”
- Clinical correlation: Swelling confined by the membrane explains localized perineal pain without spread.
Q5. What lies above the perineal membrane at this level?
A
- Sphincter urethrae attaches above the perineal membrane.
- EXAM LOCK: “Sphincter urethrae above perineal membrane.”
- Clinical correlation: Voiding discomfort after pelvic trauma suggests involvement above the membrane.
Q6. How does this region relate to the ischioanal fossa?
A
- Between the perineal membrane and the obturator foramen, the ischiopubic ramus forms the wall of the anterior recess of the ischioanal fossa.
- EXAM LOCK: “Ischiopubic ramus = wall of anterior ischioanal recess.”
- Clinical correlation: Blood tracks into this recess → deep perineal pain without obvious superficial swelling.
Q7. What happens on the ischium medial surface regarding the pudendal canal?
A
- Obturator internus arises from the inner surface of the ischium and adjacent pelvic surfaces.
- The obturator internus fascia attaches around the muscle and splits to form the pudendal canal just above the falciform ridge on the ischial tuberosity.
- The falciform ridge curves forward from the tuberosity and receives the falciform process of the sacrotuberous ligament.
- EXAM LOCK: “OI fascia splits → pudendal canal above falciform ridge.”
- Clinical correlation: Compression here → perineal sensory changes and genital pain.
Q8. Which muscles anchor near the ischial spine on the inner surface?
A
- Levator ani and coccygeus attach to the inner surface of the ischial spine.
- EXAM LOCK: “Ischial spine (inner) → levator ani + coccygeus.”
- Clinical correlation: Injury near the spine worsens pelvic floor instability and defecatory pain.
Reply “next” for Segment 14 (Sex differences on a dry hip bone + exam identification logic).
Hip Bone (Innominate) — SARR
Segment 14 — Sex differences on a dry hip bone (exam + forensic logic)
Q1. Why does the female pelvis look different overall?
A
- The iliac ala is drawn outward in females to widen the pelvis for childbirth.
- EXAM LOCK: “Female pelvis = laterally flared iliac ala.”
- Clinical correlation: Lateral flare increases pelvic inlet/outlet capacity.
Q2. What is the single most reliable dry-bone feature for sexing?
A
- Greater sciatic notch:
- Female: wide, near right angle
- Male: narrow, sharply angled
- EXAM LOCK: “Wide ≈ right angle notch = female.”
- Clinical correlation: This feature alone often suffices in OSCEs.
Q3. What is the preauricular sulcus, and who has it?
A
- A groove below the arcuate line near the auricular surface.
- Common in females, related to ligamentous stress of pregnancy.
- EXAM LOCK: “Preauricular sulcus → female pelvis.”
- Clinical correlation: Supports parity-related pelvic remodeling.
Q4. How does the ischial spine differ?
A
- Female: spine lies in the plane of the ischial body (less medial projection).
- Male: spine projects medially, narrowing the outlet.
- EXAM LOCK: “Non-projecting spine = female.”
- Clinical correlation: Outlet width is critical for delivery mechanics.
Q5. What about the obturator foramen shape?
A
- Female: triangular
- Male: oval
- EXAM LOCK: “Triangle = female; oval = male.”
- Clinical correlation: A supportive, not solitary, discriminator.
Q6. What metric relationship clinches the diagnosis?
A
- Distance pubic symphysis → anterior acetabular margin:
- Female: greater than acetabular diameter
- Male: equal to or less than acetabular diameter
- EXAM LOCK: “Pubis→acetabulum distance > acetabular diameter = female.”
- Clinical correlation: Reflects elongated anterior pelvic segment in females.
Q7. Integrated OSCE wrap-up (how to answer fast)
A
- Findings pointing to female pelvis:
- Laterally flared iliac ala
- Greater sciatic notch ≈ right angle
- Preauricular sulcus present
- Ischial spine not inverted
- Obturator foramen triangular
- Pubis→acetabulum distance > acetabular diameter
- EXAM LOCK (one-liner):
“Wide sciatic notch, non-projecting ischial spine, triangular obturator foramen, preauricular sulcus, and a longer pubic segment indicate a female pelvis.”
Reply “next” for Segment 15 (Ossification timeline of the hip bone—ages you must know).
Hip Bone (Innominate) — SARR
Segment 15 — Ossification timeline of the hip bone (ages you must know)




Q1. How does the hip bone develop—bone or cartilage first?
A
- The hip bone develops in cartilage.
- EXAM LOCK: “Hip bone = cartilaginous model first.”
- Clinical correlation: Pediatric X-rays show cartilage gaps that are normal, not fractures.
Q2. What are the primary ossification centres and when do they appear?
A
- Three primary centres, all near the acetabulum:
- Ilium → 2nd month of fetal life (first; main weight-bearer)
- Ischium → 3rd month
- Pubis → 4th month
- EXAM LOCK: “Ilium 2nd, Ischium 3rd, Pubis 4th fetal month.”
- Clinical correlation: Relative size at birth reflects this order (ilium largest).
Q3. What does the hip bone look like at birth?
A
- Acetabulum is wholly cartilaginous.
- Ilium appears as a broad bony blade.
- Ischium + pubis are tiny bony bars buried in cartilage.
- EXAM LOCK: “Cartilage acetabulum at birth; ilium big, pubis/ischium small.”
- Clinical correlation: Apparent acetabular “defects” on neonatal imaging are physiological.
Q4. What is the triradiate (Y-shaped) cartilage, and why is it critical?
A
- The ilium, ischium, and pubis approach each other but remain separated by Y-shaped cartilage within the acetabulum.
- EXAM LOCK: “Three bones meet via triradiate cartilage.”
- Clinical correlation:
- Injury or premature fusion → shallow acetabulum, hip dysplasia, early OA.
Q5. What fuses around 7 years, and why is this a trap?
A
- Ischial ramus + pubic ramus fuse at about 7 years.
- EXAM LOCK: “Ischiopubic rami fuse ≈ 7 years.”
- Clinical correlation: Lucent line here in a child ≠ fracture; avoid over-diagnosis.
Q6. What happens around 8 years?
A
- Secondary ossification centres appear in the acetabular cartilage.
- EXAM LOCK: “Secondary acetabular centres ≈ 8 years.”
- Clinical correlation: Damage at this stage can distort socket development.
Q7. When is acetabular ossification complete?
A
- By about 18 years, ossification across the acetabulum is complete and the triradiate cartilage disappears.
- EXAM LOCK: “Acetabulum complete ≈ 18 years.”
- Clinical correlation: Persistent triradiate cartilage suggests skeletal immaturity.
Q8. What about the secondary centres around the periphery?
A
- Multiple secondary centres (e.g., iliac crest, ischial tuberosity) appear during adolescence.
- They fuse with the main bone by ~25 years.
- EXAM LOCK: “Peripheral centres fuse ≈ 25 years.”
- Clinical correlation: Useful for age estimation in orthopedics/forensics.
Q9. One-line examiner synthesis
A
“The hip bone ossifies from three primary centres (ilium 2nd, ischium 3rd, pubis 4th fetal month); the acetabulum is cartilaginous at birth with triradiate cartilage, ischiopubic rami fuse at 7 years, secondary acetabular centres appear at 8 years, acetabular ossification completes by 18 years, and peripheral centres fuse by about 25 years.”
If you want, say “wrap” for a single-page exam recap, or “MCQs” for high-discriminator questions from this chapter.